Poster Title
Untangling the Mystery: Radiological Insights into Female Pelvic Organ Torsion
Authors
Lawson B, Shakur A, Lee J, Buckley A, Makaza R, Jimenez-Linan M, Rajendran I, Smith J, Addley H, Freeman S.
Teaching Objectives
Review of the topic
Definition
Torsion is the twisting of an organ, or part of an organ, along its own length.
Clinical Symptoms
Patients classically describe sudden onset severe abdominal / pelvic pain and vomiting but symptoms may be vague.
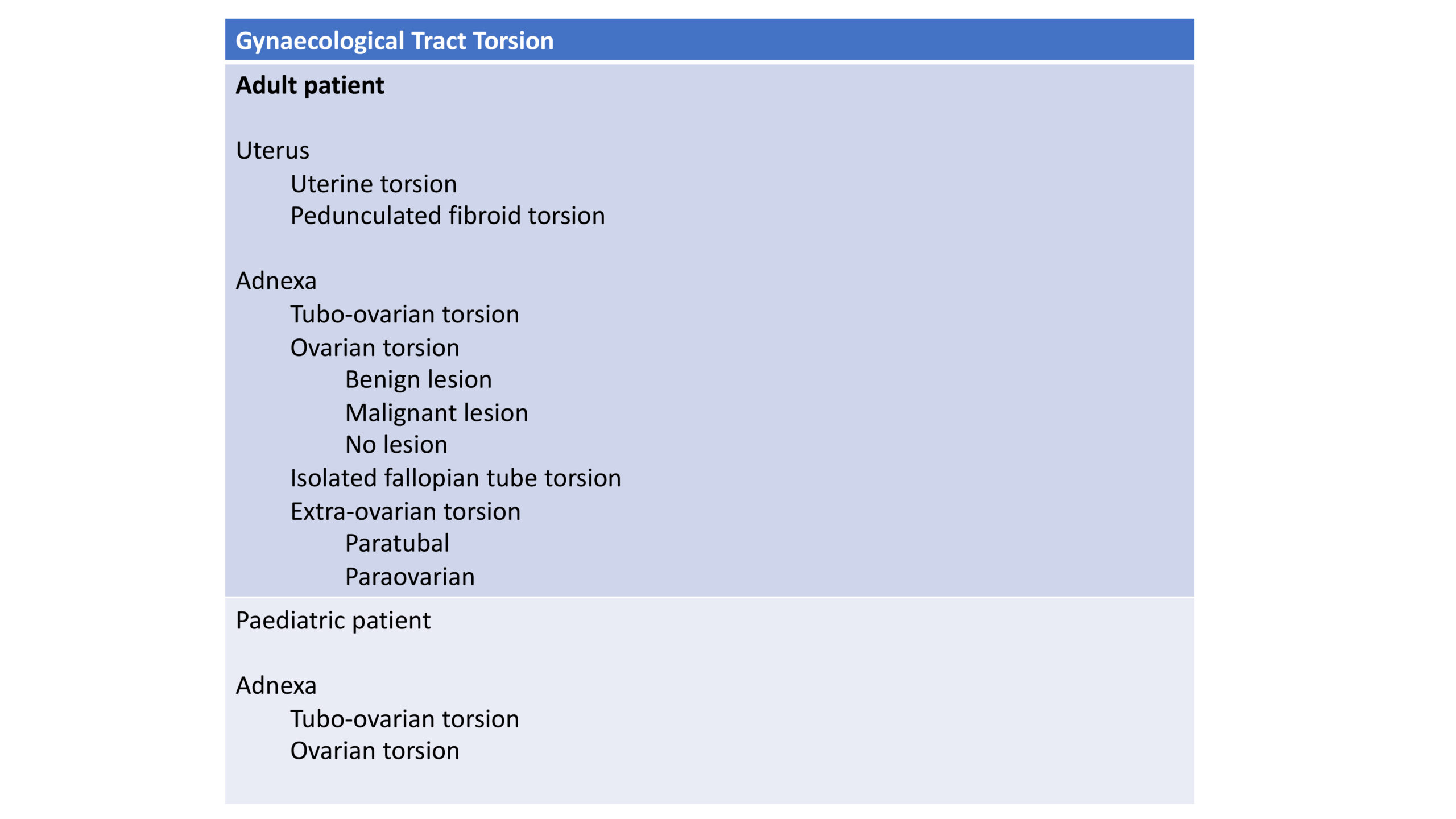
Subtypes of Female Pelvic Organ Torsion
Please see table 1.
Imaging Findings
Adults
Uterine torsion is rare and is defined as a rotation of >45° around the long axis of the uterus and usually occurs at the level of the uterine isthmus at the junction of uterine body and cervix. It has most commonly been reported in cases of pregnancy and underlying congenital uterine anomalies (1). Uterine leiomyomas, pelvic adhesions and adnexal masses are other predisposing factors. Presenting complaints and clinical examination findings are often non-specific. Characteristic imaging findings include the “whirl sign” centred on the cervix.
Ultrasound
CT
MRI
Teaching point 1: Uterine torsion is defined as rotation of > 45° around the long axis of the uterus. Although rare, it has been reported in women of all ages, from premenarchal to postmenopausal stages. According to the literature, in older menstruating women or postmenopausal women, uterine leiomyomas are the most common predisposing factor for uterine torsion.
Pedunculated subserosal fibroid
More commonly, torsion of a pedunculated subserosal fibroid presents with acute pain. On CT, a mass connects to a normal uterus via a stalk. In comparison with ovarian torsion where the twisted pedicle is thick, the twisted pedicle of a pedunculated subserosal fibroid is thin and sometime difficult to identify on CT (5). On ultrasound, a thin stalk may be seen connecting a mass to the uterus. Depending on the degree of ischaemia, there can be decreased vascularity within the mass. MRI demonstrates a whirl in the fibroid pedicle with reduced enhancement or necrosis. Complications include peritonitis or avulsion of the fibroid (as in image 1, Case 2).
Adnexal torsion of the ovary, fallopian tube or both tube and ovary, most commonly occurs secondary to an underlying benign ovarian lesion, with lesions greater than 5 cm in diameter with a particularly increased risk of torsion. The commonest lesions include mature cystic teratomas and physiological cysts / serous cystadenomas (image 3). Ovulation induction for infertility stimulates the production of multiple follicular cysts, resulting in ovarian enlargement and increased susceptibility for torsion. Additional risk factors include pregnancy, particularly in the first trimester when corpus luteum cysts may develop (6). Adhesions in malignancy and endometriosis reduce the risk of torsion (7) although image 4 illustrates some examples of torsion in association with borderline and malignant change. Radiological features include ovarian enlargement, displacement of the ovary superiorly into the midline and uterine deviation towards the affected side.
Ultrasound
CT
MRI
Teaching point 2: Dermoid cysts are considered a relatively common cause of adnexal torsion, reported in up to 25% of torsion cases. The pathophysiology of dermoid cysts causing adnexal torsion is hypothesized to be the fatty content of the cyst, leading to its “floatation” outside the pelvis.
Teaching point 3: Ovarian fibromas / thecomas are benign tumours arising from mesenchymal spindle cells which produce collagen. They account for only 4% of all ovarian neoplasms but are the most common solid primary ovarian tumour in asymptomatic women of all ages. They can however undergo torsion with resultant necrosis and inflammation resulting in elevated Ca125.
Teaching point 4: In benign ovarian torsion, internal haemorrhage can be mistaken for enhancing soft tissue on CT and lead to a false positive diagnosis of malignancy. In addition, the appearance of an underlying benign ovarian lesion may change following torsion (9, 10).
Teaching point 5: According to the literature, adhesions related to malignant lesions and endometriosis are believed to be protective. A case report by Vicente et al. describes a case of an ovarian borderline tumour presenting as ovarian torsion in a 17-year-old patient. Torsion is reported in 1.1 – 2.0 % of malignant ovarian neoplasms. A 15-year analysis of 707 patients with proven ovarian torsion reported 13 malignancies, 4 borderline tumours and 2 undifferentiated adenocarcinomas. Malignant tumours are a rare underlying cause of torsion, but failure to suspect or detect a malignant tumour may compromise patient prognosis as the patient may not be offered the best surgical option at the start (11).
Isolated fallopian tube torsion is less common and may be secondary to paratubal cysts. It primarily affects adolescents and ovulating women, and most commonly affects the right side, possibly because of partial immobilisation of the left tube by its proximity to the sigmoid mesentery (12). Intrinsic risk factors include pelvic inflammatory disease, hydrosalpinx, tubal ligation and tubal neoplasm. Extrinsic risk factors include adhesions, adnexal venous congestion, adjacent ovarian or paraovarian masses, uterine masses, gravid uterus and trauma (13). Complications include fallopian tube necrosis and gangrenous transformation, leading to increased risk of superinfection and peritonitis (14). Local necrosis can also result in irreversible damage to ipsilateral ovary (15). Please see images 5, 6, 7, 8.
Ultrasound
CT / MRI
Teaching Point6: Although ovarian torsion with associated tubal torsion is far more common than isolated tubal torsion, the imaging diagnosis of an isolated tubal torsion is far more difficult because of the lack of specific findings. Risk factors for isolated fallopian tube torsion include both intrinsic factors, including pelvic inflammatory disease, hydrosalpinx, tubal ligation and tubal neoplasm; and extrinsic risk factors such as adhesions, adnexal venous congestion, adjacent ovarian and paraovarian masses, uterine masses, gravid uterus and trauma.
Paediatric
Adnexal torsion may occur due to a coexistent mass or ligamentous laxity with a normal ovary. Venous congestion and ischaemia cause oedema and haemorrhage, resulting in hyperechoic ovarian stroma with peripherally located follicles. Adnexal masses increase the weight of the ovary and predispose it to torsion. In a study by Oltmann et al, adnexal masses were identified in 54 % of paediatric adnexal torsion cases. Benign ovarian neoplasms occurred in 19% of cases, with mature cystic teratoma being the most frequent lesion seen (16). The primary imaging modality is ultrasound as it is readily available and does not require use of ionizing radiation. Please see images 9 and 10.
Ultrasound
CT
MRI
Teaching point 7: Common imaging findings in the prepubescent and adolescent population include asymmetrical enlargement of the ovary, peripheral location of the ovarian follicles, and midline location of the ovary. In premenarchal patients who are diagnosed with adnexal torsion, the underlying pathogenic process may be related to elongation of the utero-ovarian ligaments, and the ovary itself is more likely not to have underlying pathology compared with the ovaries in older women (18).
Img description:
Table 1: Subtypes of Gynaecological Tract Torsion
Img description:
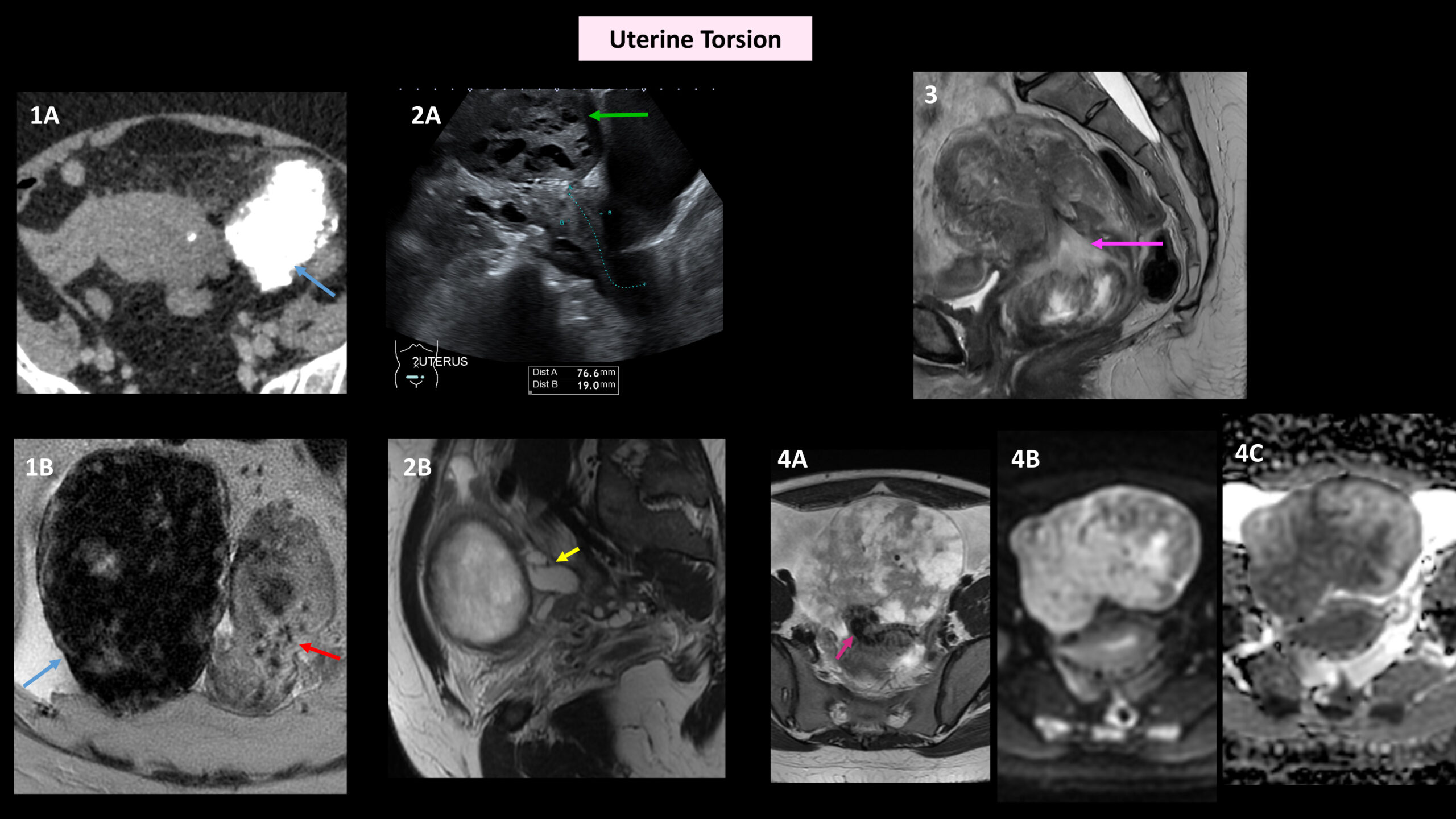
Image 1: Uterine torsion.
Case 1: A 69-year-old female presented with lower abdominal pain. Initial imaging with contrast-enhanced CT (image 1A, blue arrow) demonstrated a large 10 cm calcified pedunculated fibroid arising from the left lateral wall of the uterus. MRI was carried out four days after baseline imaging because of ongoing symptoms. The pedunculated uterine fibroid was now to the right of midline (image 1B, coronal T2, blue arrow). The uterus was bulky, with high T2 signal noted throughout the myometrium. There was a twist in the uterus at the cervico-uterine junction (image 1B, axial T2, red arrow). Appearances were compatible with uterine torsion.
Case 2: A 45-year-old patient with intermittent diarrhoea and abdominal bloating had ultrasound scan which showed multiple subserosal uterine fibroids. Anterior to the uterus and above the urinary bladder (image 2A, green arrow) there was a large heterogeneous mass which measured 10cm, with cystic areas but no internal vascularity. There was possible subtle attachment to the fundus of the uterus, difficult to visualise on ultrasound. This lesion was thought to represent a large pedunculated fibroid which had undergone cystic degeneration and possible torsion. On MRI, there was a corresponding 13cm complex heterogeneous cystic mass containing haemorrhagic products. Best seen on sagittal T2 (image 2B) there was a serpiginous structure (yellow arrow), with evidence of a swirl, posterior to the mass likely to represent a dilated torted haematosalpinx. At laparoscopy, there was enlarged 12-week size parasitic fibroid with no connection to the uterus and sitting above the uterus, likely to represent a pedunculated fibroid which had undergone torsion and become detached. The fibroid was also attached to both fallopian tubes, which were unusually torted around each other by the mass.
Case 3: A postmenopausal woman with suspected endometrial cancer and with persistent heavy bleeding and two negative hysteroscopy and biopsy results had an MRI for further evaluation. Sagittal T2 (image 3) demonstrated a bilobed submucosal fibroid arising from the posterior uterine body measuring 9.5cm, which prolapsed through the endocervical canal into the vagina. The narrow portion of the fibroid had a swirl (purple arrow) in keeping with torsion. The fibroid was heterogeneous in keeping with myxoid degeneration. Blood products within the endometrial cavity made assessment of endometrial thickness difficult. This case highlights how torsion of the submucosal fibroid resulted in difficulty in obtaining both histological and radiological diagnosis.
Case 4: A 40-year-old female with chronic pelvic pain had an MRI which showed an anteverted uterus and a large anterior midline mass, with bridging vessels to the uterine fundus, in keeping with a large pedunculated subserosal fibroid. The fibroid measured 11cm. Multiple areas of high T2 signal intensity were in keeping with cystic degeneration of the fibroid (image 4A, Axial T2). Torsion of the pedicle of the fibroid was also seen (pink arrow). Whilst there was no internal haemorrhage, the fibroid demonstrated marked restricted diffusion (image 4B, high b-value DWI and image 4C, ADC map). The patient underwent laparoscopic myomectomy. Histopathology showed smooth muscle tumour of uncertain malignant potential (STUMP) – therefore further discussion at the Gynaecology Oncology MDT was arranged.
Img description:
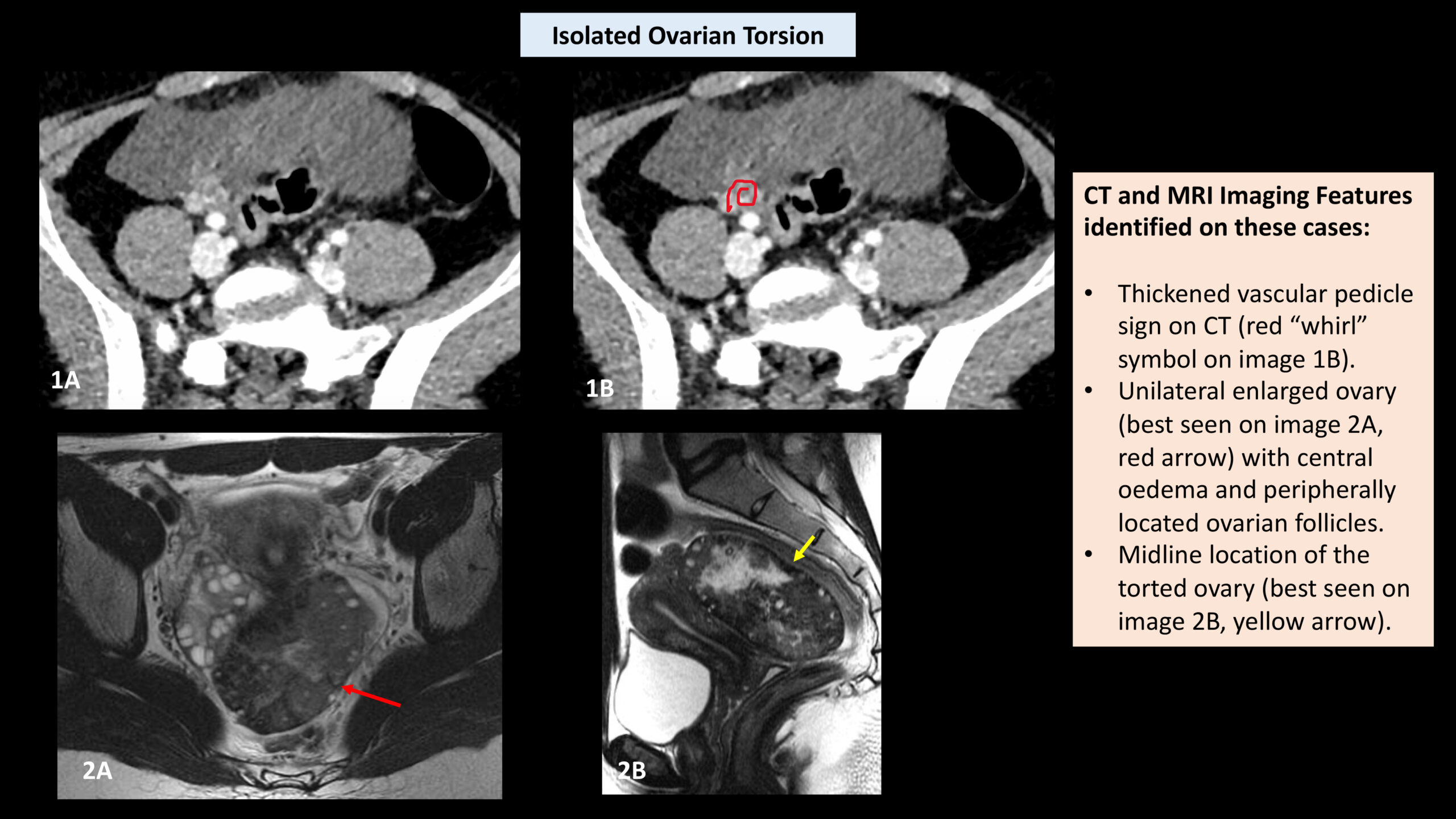
Image 2 – Isolated Ovarian Torsion
Case 1: (images A and B, Axial portal venous phase CT) and case 2 (image A, Axial T2 MRI and image B, Sagittal T2 MRI) are two different cases which depict the typical CT and MRI features of isolated ovarian torsion. Imaging findings include a unilateral enlarged ovary (> 4cm) (as indicated on image 2A, red arrow), midline location (either superior to uterine fundus or in the Pouch of Douglas, as in image 2B), peripherally displaced follicles, ovarian stroma oedema (low attenuation central in case 1, image A and high signal intensity in Case 2), the thickened vascular pedicle sign on CT (as indicated by the red “whirl” symbol in image 1B) and the whirlpool sign of the ovarian pedicle on MRI.
Img description:
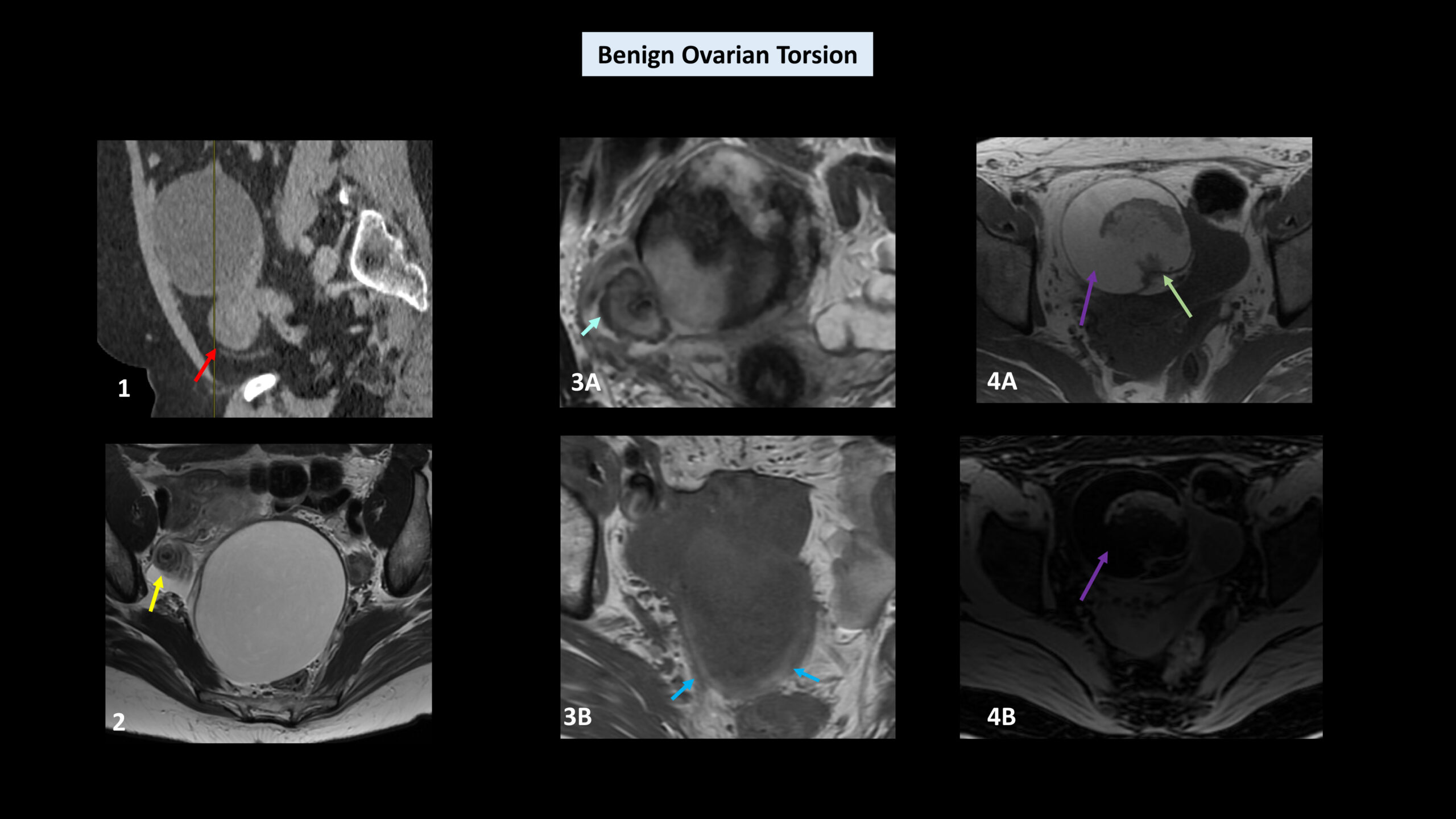
Image 3 – Benign Ovarian Torsion:
Case 1: Image 1 is sagittal reformat of a contrast-enhanced CT carried which demonstrated a 13cm cystic lesion lying anterior to the uterus in an unusual anatomical position, with a “twisted pedicle sign” (red arrow). Appearances were highly concerning for left ovarian torsion secondary to the large cystic mass. At laparoscopy, the left ovarian cyst was torted twice with the fallopian tube, the cyst reaching 18 weeks’ size. Histopathology sections from the ovarian cyst wall and fallopian tube were extensively haemorrhagic and necrotic, and whilst the appearances were in keeping with the clinical history of torsion of an ovarian cyst, due to lack of epithelial lining, it was not possible to comment on the nature of the cyst.
Case 2: Image 2 depicts an Axial T2 MRI demonstrating the whirlpool sign of a torted right ovarian pedicle (yellow arrow) secondary to torsion of a right ovarian simple cyst.
Case 3: Image 3A is an Axial T2 MRI demonstrating a heterogeneous 8cm mass arising from the right ovary, with a twist in the right ovarian pedicle (light blue arrow). A peripheral rim of high T1 signal (image 3B, dark blue arrows) is in keeping with haemorrhage. Even with the oedema, the lesion was iso-hypointense relative to the myometrium, a finding strongly suggestive of fibromas (as opposed to malignant masses). The patient underwent laparoscopic bilateral salpingo-oophorectomy and pathology confirmed an infarcted ovarian fibroma.
Case 4: Image 4A is an Axial T1 image of a 50-year-old female who presented to her GP following pain during intercourse. She had an ultrasound which showed a left adnexal mass so proceeded with MRI. MRI demonstrates torsion of a left ovarian mature teratoma with an internal Rokitansky nodule (green arrow), internal fat content (purple arrow) and a swirl in the left ovarian pedicle (not shown). Axial T1 FS (image 4B) demonstrates loss of signal of the internal fat content. Histopathology confirmed mature teratoma of the left ovary.
Img description:
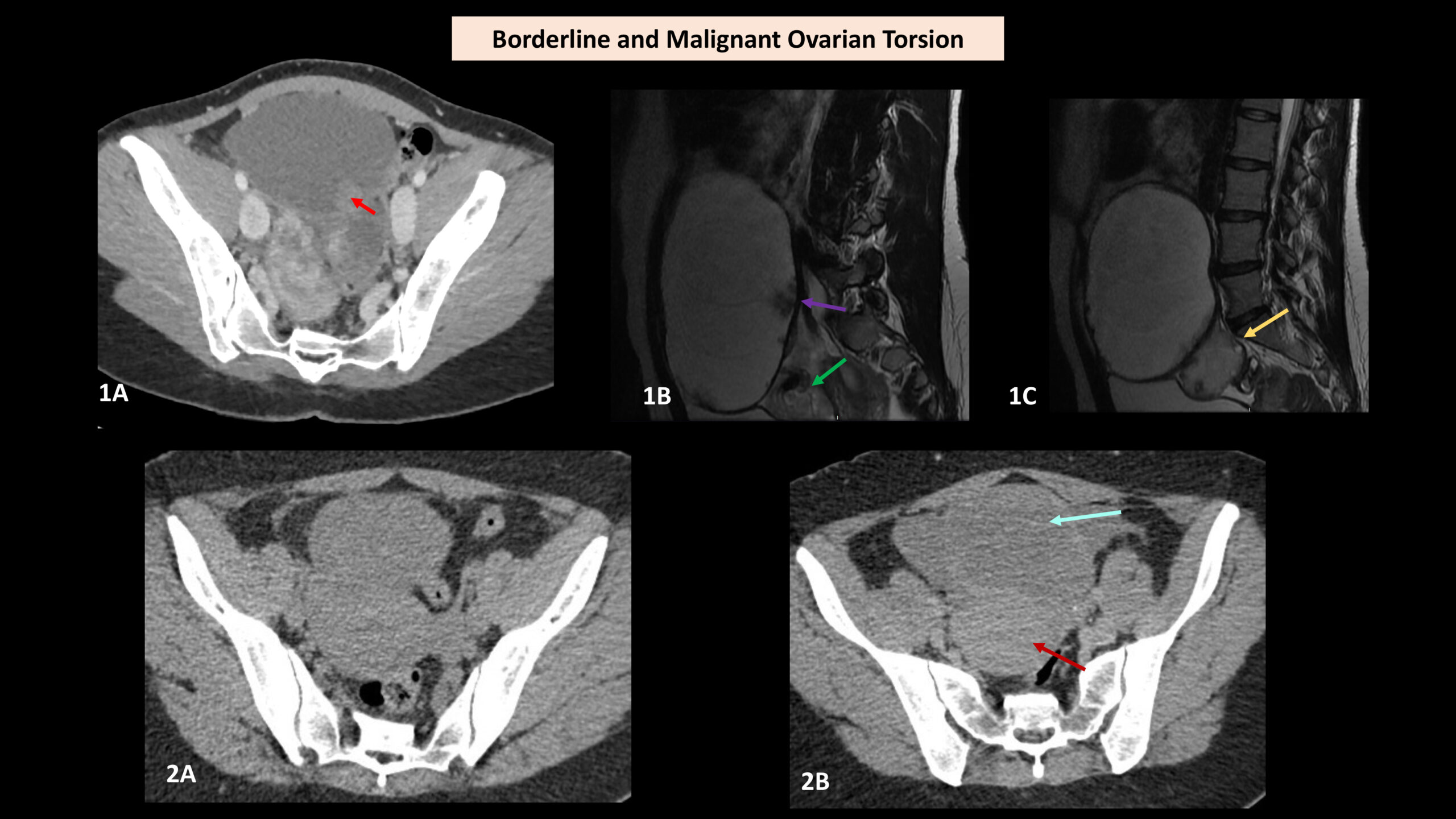
Image 4 – Borderline and Malignant Ovarian Torsion
Case 1: Post contrast CT acquisition in portal venous phase (image 1A) demonstrates a swirl in the right ovarian pedicle consistent with torsion. Peripheral soft tissue nodularity is seen within the large right ovarian cyst (red arrow). On MRI (images 1B and 1C – Sagittal T2 images) these nodules correspond to multiple papillary lesions (image 1B, purple arrow), highly suspicious for a serous borderline tumour. A swirl in the pedicle is seen more inferiorly on image 1B (green arrow). The cyst arises relatively exophytically from the ovary which is oedematous with peripherally placed follicles (image 1C, yellow arrow). The patient underwent a laparotomy and right sided ovarian cystectomy with omental biopsy. At surgery, the ovary was torted three times around the pedicle. Pathology confirmed a right ovarian borderline serous tumour.
Case 2: A 60-year-old female presented with acute right renal colic. A non-contrast CT Renal (image 2A) showed no ureteric stone but the presence of a “fibroid” uterus. A CT Urogram carried out 24 hours later (image 2B) showed a part cystic/part solid mass (blue arrow) at the midline pelvis separate to the uterus (red arrow) and an increase in the volume of intraperitoneal free fluid. Surgery and pathology confirmed clear cell carcinoma causing right ovarian torsion.
Img description:
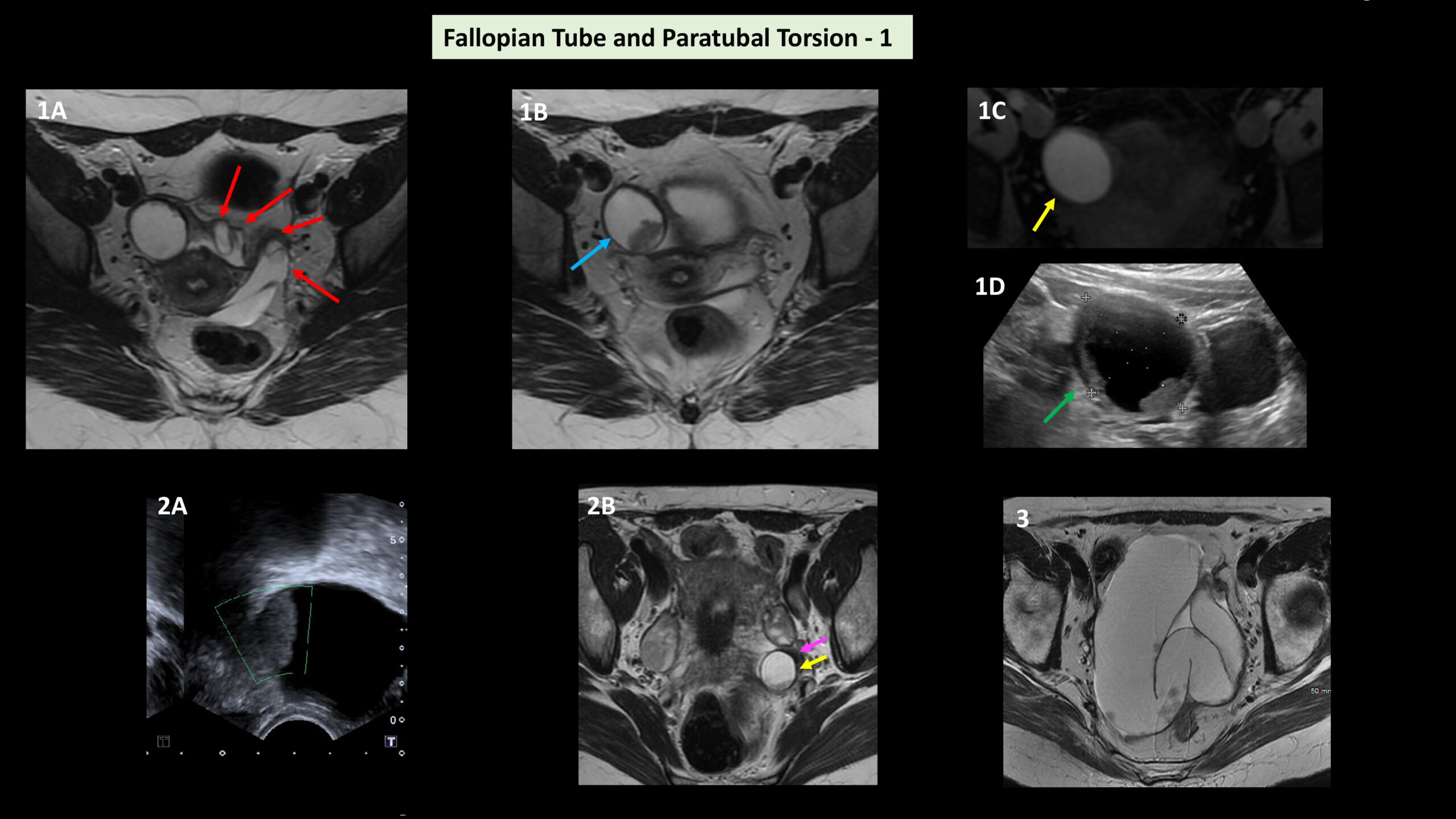
Image 5 – Fallopian Tube and Paratubal Torsion (1):
Case 1: This 17-year-old female had an MRI for further assessment of a persistent cyst on ultrasound. MRI demonstrated torsion of the left fallopian tube, which was twisted four times (images 1A, Axial T2, red arrows), secondary to a fimbrial haemorrhagic cyst lead point which demonstrated high signal intensity on both T2 and T1 FS (image 1B, Axial T2, blue arrow and image 1C, Axial T1 FS, yellow arrow). The fimbrial cyst corresponds to the cystic structure containing internal debris/blood clot that had been seen on previous ultrasound scans (image 1D, green arrow).
Case 2: This 46-year-old female patient presented with left iliac fossa pain. Ultrasound imaging (image 2A) showed an enlarged left ovary (volume 60 mL), containing a 43 mm cyst with an avascular soft tissue component measuring 24mm. MRI demonstrated the cyst to be posterior to, and separate from, the normal left ovary (yellow arrow, images 2B, Axial T2) with a tiny swirl between the ovary and the cyst (purple arrow). It measured 22 x 20 x 22 mm and demonstrated high signal on T1 and T1 FS in keeping with internal blood products. Appearances were in keeping with haemorrhagic infarction of a torted fimbrial/paraovarian cyst. Case 3: Image 3 is an Axial T2 image demonstrating an enlarged torted fallopian tube containing multiple papillary solid components in keeping with fallopian tube malignancy.
Img description:
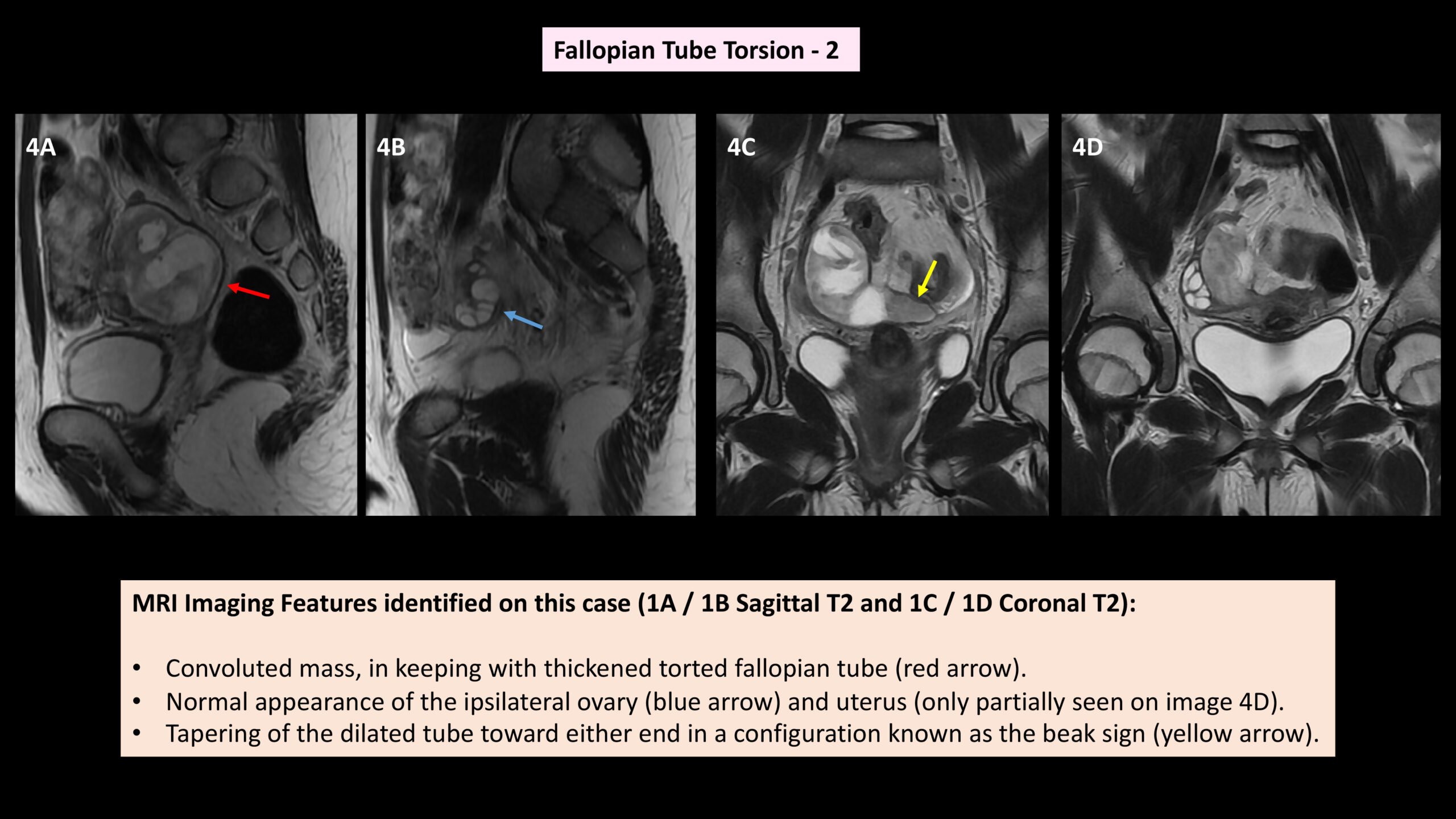
Image 6 - Fallopian Tube Torsion (2) - MRI images illustrating key imaging features.
Img description:
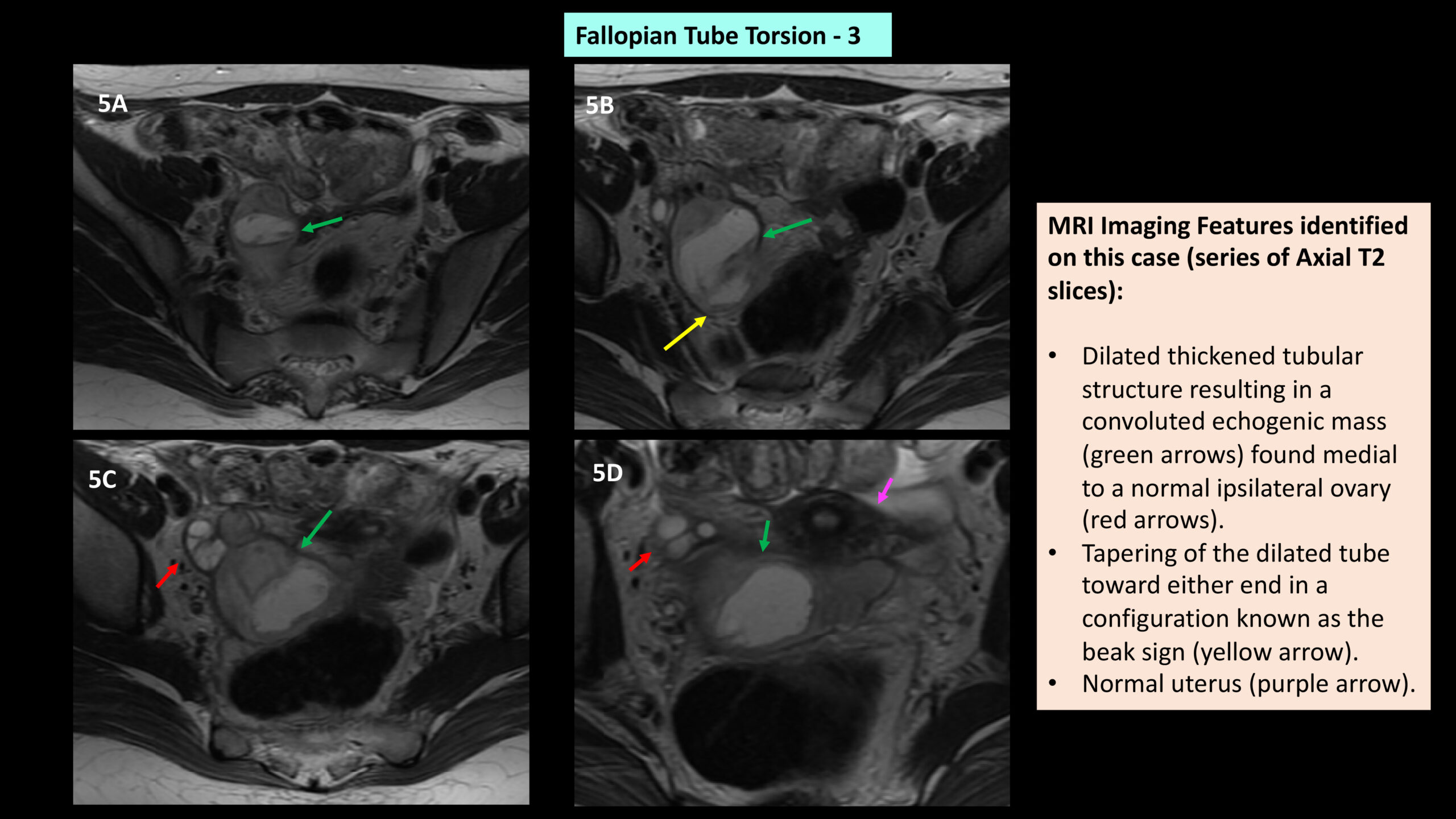
Image 7 - Fallopian Tube Torsion (3) - MRI images illustrating key imaging features.
Img description:
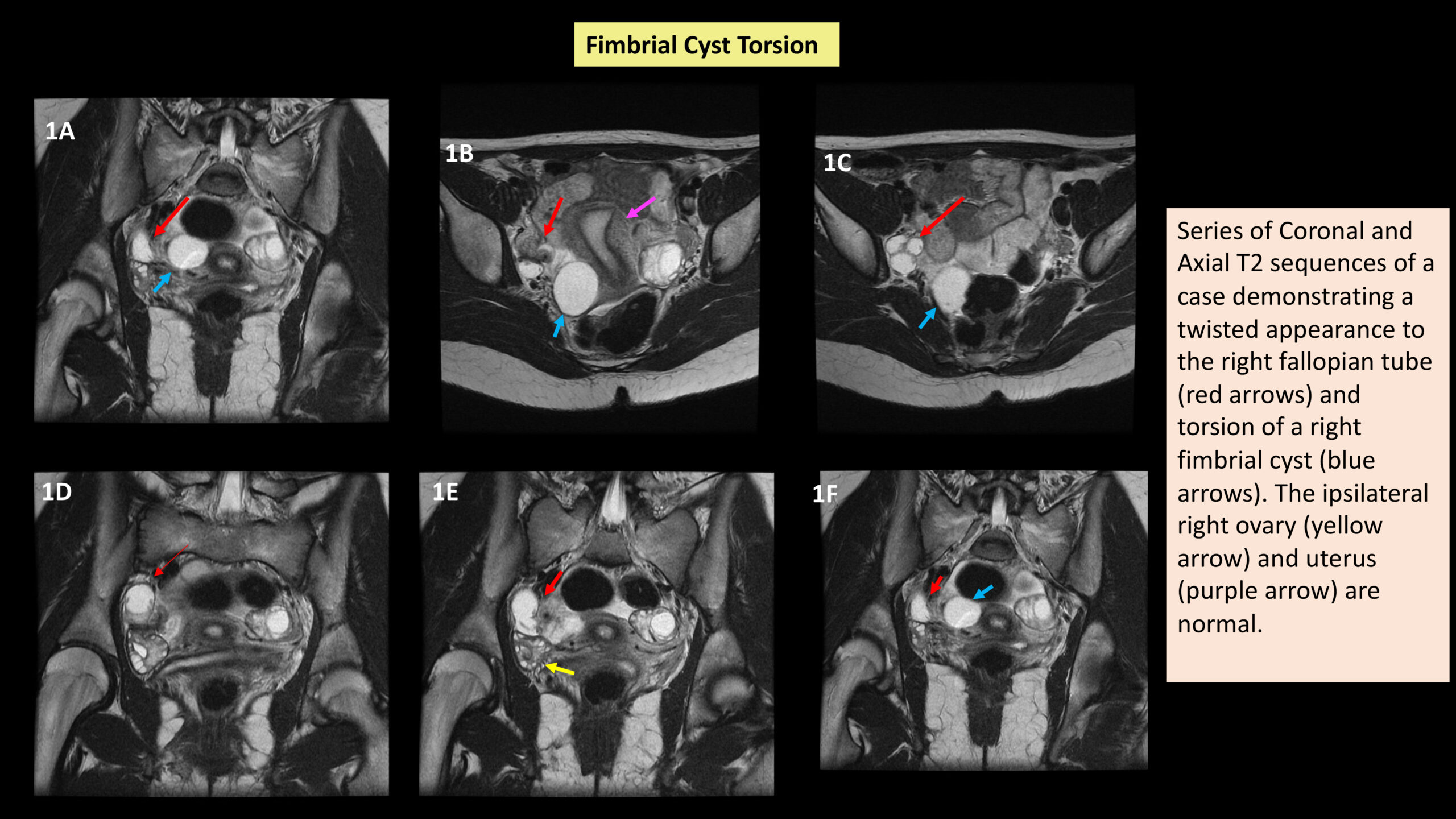
Image 8 - Fimbrial Cyst Torsion - MRI images illustrating key imaging features.
Img description:
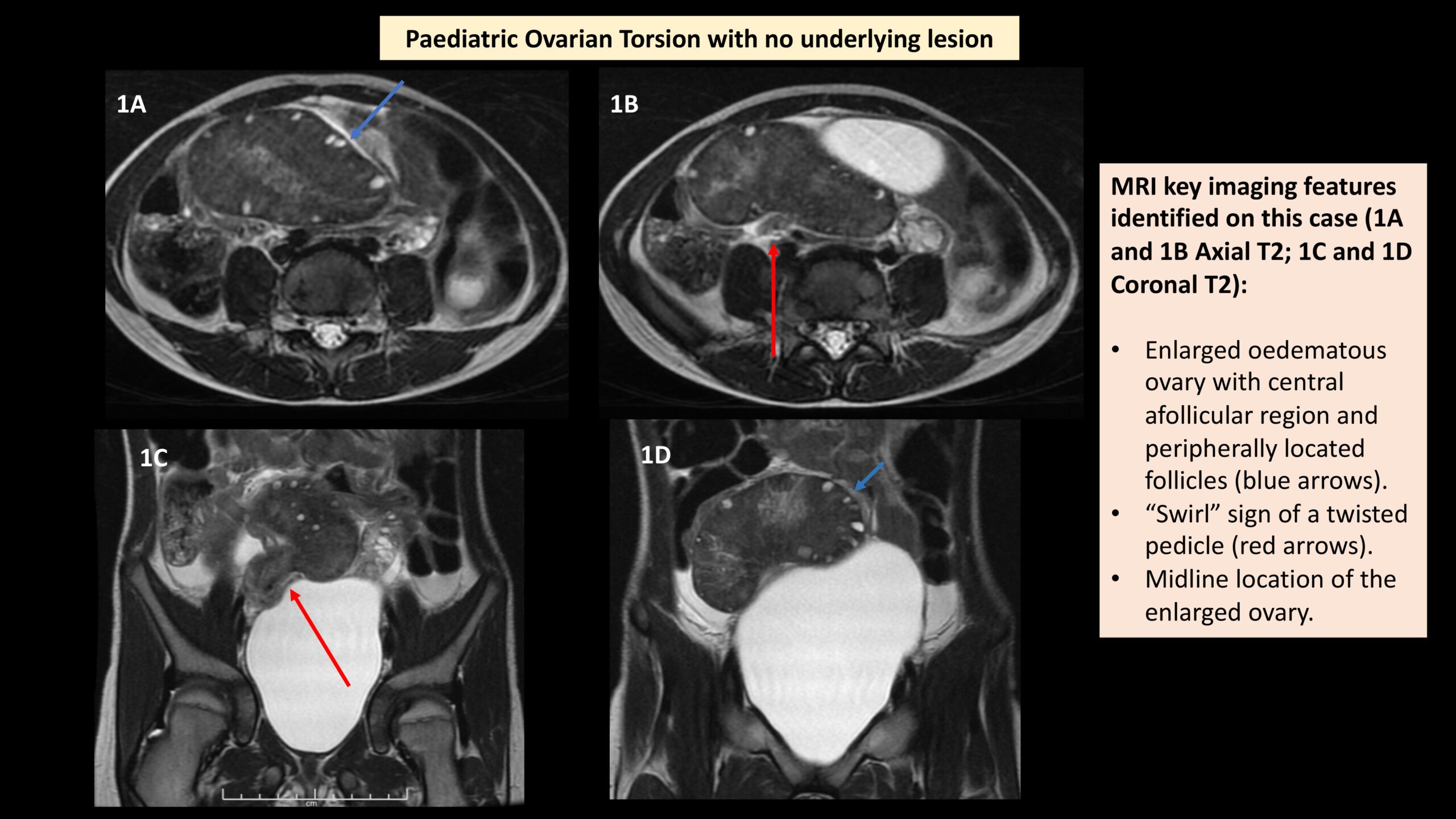
Image 9 - Paediatric ovarian torsion with no underlying lesion. MRI images illustrating key imaging features.
Img description:
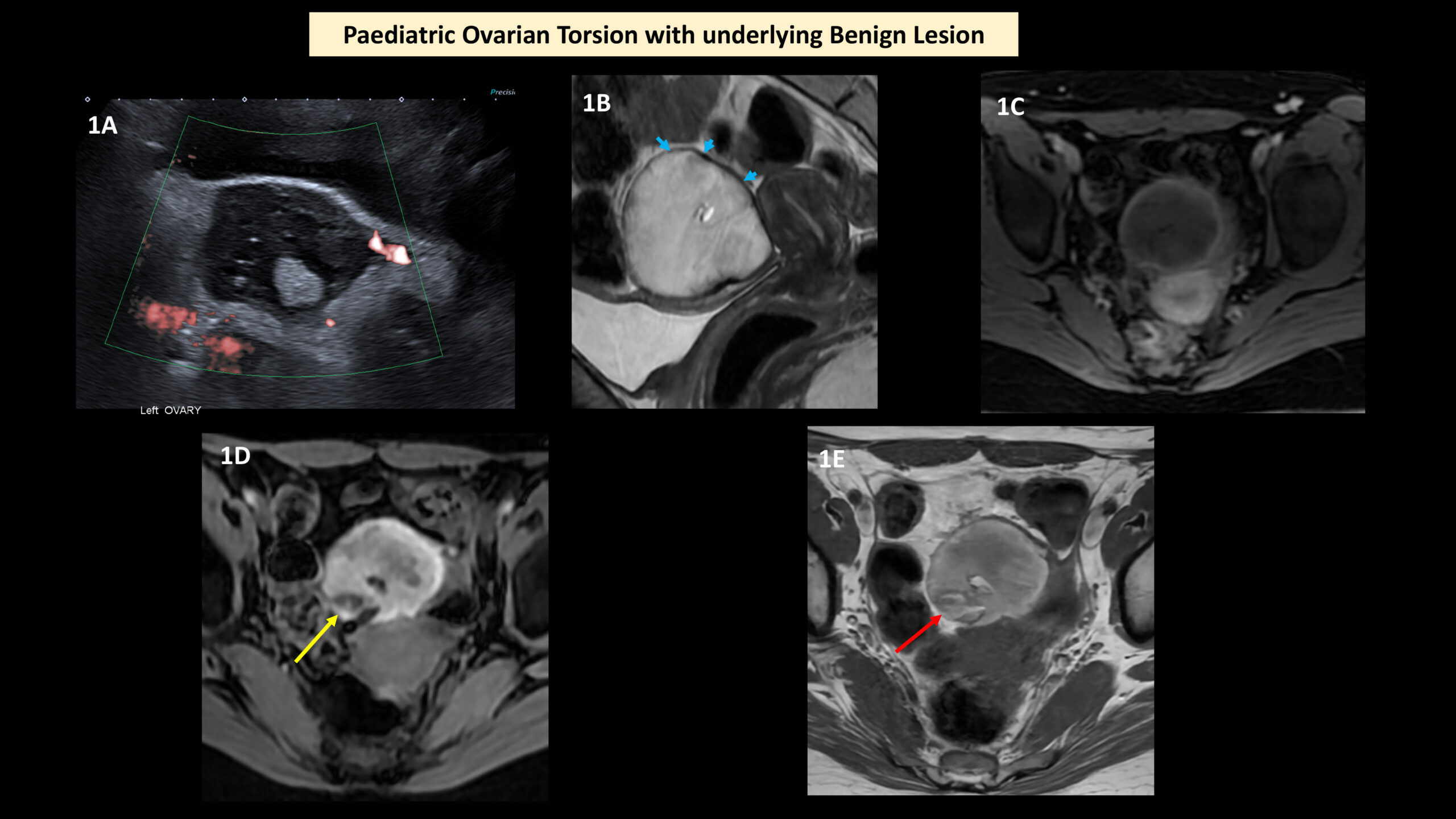
Image 10 - Paediatric ovarian torsion with underlying ovarian lesion:
Case 1: This 13-year-old female patient with a past surgical history of previous right salpingo-oophorectomy for ovarian mature teratoma presented to the emergency department with acute pelvic pain. Ultrasound scan (image 1A) showed an enlarged and oedematous left ovary, with reduced vascularity, raising suspicion for torsion. MRI showed a 58 mm x 50 mm x 50 mm lesion in the midline pelvis (image 1B) with internal blood degradation products (Axial T1 fat saturation sequence, image 1C) and a low signal intensity rim likely to represent haemosiderin (Sagittal T2, image 1B, blue arrows). Appearances were compatible with haemorrhagic necrosis of the left ovary secondary to torsion. A few locules of macroscopic fat were demonstrated within the lesion (T1 fat saturation sequence image 1D, yellow arrow and Axial T1 sequence image 1E, red arrow) suggestive of an underlying mature teratoma -confirmed on histopathology.
Conclusion
Ovarian torsion secondary to a large ovarian lesion which acts as a lead point, with possible associated involvement of the ipsilateral fallopian tube, is a well known clinical entinity. However, other subtypes of female pelvic organ torsion such as uterine torsion, torsion of a pedunculated fibroid, isolated fallopian tube torsion or isolated ovarian torsion are less commonly encountered clinical entities. Our educational presentation has provided a pictorial representation of the imaging appearances of various types of gynaecological tract torsion. The severity of vascular impairment secondary to torsion depends on the degree of rotation, and as the arterial supply is compromised, haemorrhagic infarction occurs. Prompt diagnosis is essential, but non-specific symptoms make an early diagnosis of torsion challenging and results in patients undergoing a range of different radiological examinations. Patients may also present during pregnancy or have co-existing pathologies, increasing the complexity of some of these cases. A high level of clinical suspicion is warranted. Appropriate timely imaging has a fundamental role in early diagnosis and treatment to avoid devastating long-term effects. Please see image 11.
Teaching point 8: The presence of a corpus luteum cyst or ovarian hyperstimulation syndrome predisposes to ovarian torsion in the first trimester. These usually resolve in the second and third trimester, therefore ovarian torsion in the second and third trimester is rare (19).
Img description:
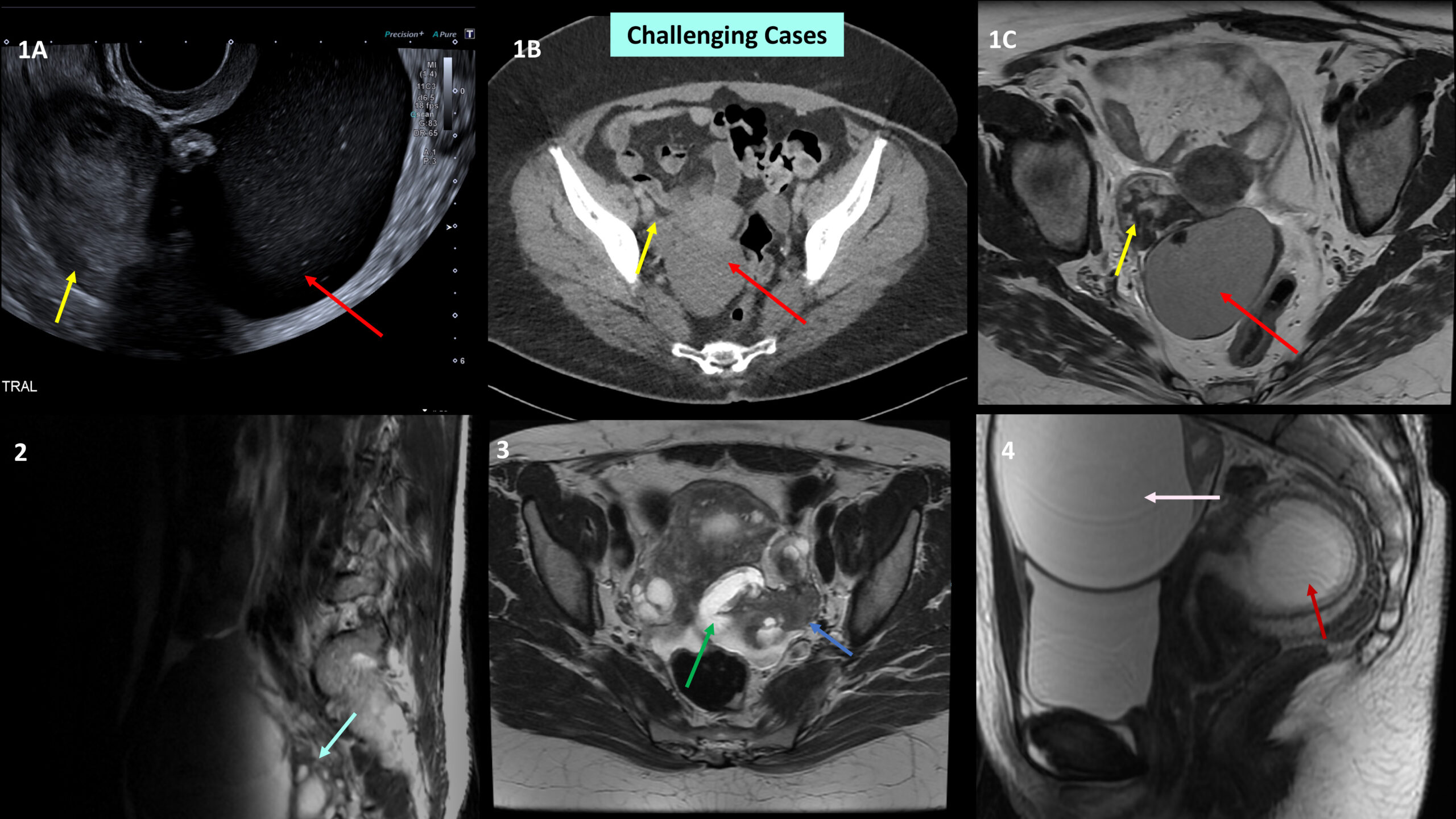
Challenging Cases:
Case 1: A 35-year-old female with a past medical history of previous intra-abdominal sepsis and right iliac fossa pain had a pelvic ultrasound scan (image 1A) which showed a 67 mm cyst at the midline with internal low-level echoes suspicious for an endometrioma (red arrow). Adjacent to the cyst, there was a 47 mm oedematous soft tissue structure with no internal vascularity (yellow arrow) suspicious for concomitant adnexal torsion. Portal venous phase CT (image 1B) demonstrates the endometrioma (red arrow) and adjacent structure (yellow arrow). No alternative cause for the pain was identified on CT. Axial T2 MRI (image 1C) confirms an endometrioma arising from the right ovary (red arrow). Within the right adnexa, lateral to the uterine body, there was a heterogeneous lesion measuring 53 mm which had an unusual configuration but was of predominantly low T2 signal (yellow arrow). It had a whirled appearance superomedially implying torsion of the right fallopian tube. The bizarre appearance was felt to represent chronicity of the torsion. This case highlights how co-existent pathology, such as the presence of an endometrioma, can make diagnosis of adjacent isolated fallopian tube torsion difficult. Also, whilst adhesions related to endometriosis have been reported as protective in the literature, this case also demonstrates that pelvic organ torsion can still occur with background endometriosis.
Case 2: A female who presented with back pain and reduced perianal sensation underwent a Lumbosacral Spine MRI. Best seen on sagittal T2 sequence (image 2) there was a lesion within the upper pelvis, anterior and cranial to the uterus, measuring up to 10 cm. The lesion was relatively high T2 signal intensity with multiple small peripheral follicles (blue arrow), with a swirl sign seen within the pedicle. Appearances were compatible with ovarian torsion. Operative findings were of left adnexal torsion and leakage from a left ovarian cyst. The patient underwent adnexal detorsion and left salpingo-oophorectomy. Pathology confirmed infarcted ovarian cyst, most likely a benign mucinous cystadenoma. This case highlights how the non-specific symptoms of female pelvic organ torsion can result in the diagnosis being made on any imaging modality.
Case 3: Axial T2 MRI (image 3) of a patient with abdominal pain found to have a large left hydrosalpinx (green arrow) which contained small layer of blood products. The left ovary was normal in appearance, but a soft tissue deposit (blue arrow) was seen between the left ovary and left fallopian tube which was felt to represent an endometriosis deposit. In addition, there was a “whirled” appearance to the distal left fallopian tube felt likely to represent torsion. The patient proceeded to laparoscopic left salpingo-oophorectomy, at surgery the left fallopian tube was torted and adherent to the Pouch of Douglas. Whilst no endometriosis deposit was identified at surgery, there were dense peritoneal adhesions in the pelvis, treated with adhesiolysis. This case highlights how co-existent pathology can make overall diagnosis and management more challenging.
Case 4: Sagittal T2 MRI (image 4) of an 8-week pregnant patient who was admitted with severe pain demonstrates a gravid uterus (red arrow) and a right ovarian simple cyst (pink arrow), the surrounding ovarian stroma being oedematous with features suspicious of torsion of the ovarian pedicle. The patient proceeded to laparoscopic detorsion and ovarian cystectomy.
References