Pelvic venous congestion syndrome (PVCS) in women: a neglected pathology
Pelvic venous congestion syndrome (PVCS) in women: a neglected pathology
Roberta Scicolone, Luca Saba
To review symptoms, etiology, the role of imaging in Pelvic venous congestion syndrome (PVCS) diagnosis and to underline the need for further research on the topic.
Chronic pelvic pain (CPP), defined as persistent or intermittent pain in the pelvis for more than 6 months, has a prevalence of up to 27% worldwide and PVCS is a common and still overlooked cause of CPP. Other symptoms of PCVS include dyspareunia, dysmenorrhea, and urinary urgency. These symptoms are aspecific and common to other gynecological (fibroids, adenomyosis, endometriosis), gastroenterological (irritable bowel syndrome, inflammatory bowel disease), musculoskeletal (pelvic girdle pain), infectious (pelvic inflammatory disease) and urinary disorders (painful bladder syndrome). Parity is a risk factor, but nulliparous women can present this condition as well. The aetiology of PVCS includes: - retro-aortic left renal vein, an anatomical variant where the left renal vein is located between the aorta and the vertebra. This condition is also called posterior Nutcracker syndrome (Fig. 1); - the compression of the left renal vein between the abdominal aorta and superior mesenteric artery with an angle on sagittal CT angiograms less than 35-39°, also known as anterior Nutcracker syndrome (Fig. 2); - pelvic venous insufficiency (PVI), consisting in excessive dilatation of the main veins located in the abdomen and pelvis, often resulting from the reversal of venous blood flow. We can distinguish left ovarian vein (LOV) insufficiency and right ovarian vein (ROV) insufficiency: • Causes of LOV insufficiency include a) absence, hypoplasia or post-thrombotic septations of suprarenal or hepatic segment of inferior vena cava (IVC); b) absence or hypoplasia of left renal vein (LRV); c) post-thrombotic septs or intraluminal webs in LRV; • Causes of ROV insufficiency include a) absence, hypoplasia or post-thrombotic septations of suprarenal or hepatic segment of IVC; b) absence or hypoplasia of right renal vein (RRV); c) atypical ROV drain; d) duplication of the ROV trunk. - left common iliac vein compression between the right common iliac artery and the lumbar spine, also known as May-Thurner syndrome (Fig. 3). Currently, there is no consensus on diagnostic algorithms, nor the treatment management. Ultrasonography (US) is considered the first line imaging study; with diagnostic criteria including: 5 mm threshold for ovarian and parauterine veins; a threshold of more than four dilated (>4 mm) ovarian and parauterine veins; the presence of dilated venous connections (trans-uterine veins) between left and right uterine veins; reverse venous flow during Valsalva maneuver. Computed tomography (CT) can detect dilated veins but implies exposure to ionizing radiations and does not deliver sufficient blood flow information, compared to the other imaging techniques. Magnetic Resonance (MR) with time resolved imaging (TRI) can assess blood flow dynamics and can aid in differential diagnosis owing to the excellent soft-tissue contrast, without the use of radiation and therefore safer in younger women. The criteria for CT and MR with TRI diagnosis of PVCS proposed by Coakley are: ≥ 4 ipsilateral parauterine veins of varying size; one of them showing >4 mm in diameter or the ovarian vein measuring > 8 mm. Venography remains the gold standard but invasive and normally reserved for patients who are selected for interventional treatment, the latter usually consisting in the application of a stent for the vascular obstruction, ovarian veins coiling or venous embolization for the pelvic vein varicosities. Example of a patient, presenting with flank pain, pelvic pain and hematuria, later diagnosed with PVCS due to posterior Nutcracker syndrome, is shown in Fig. 4, 5 and 6.
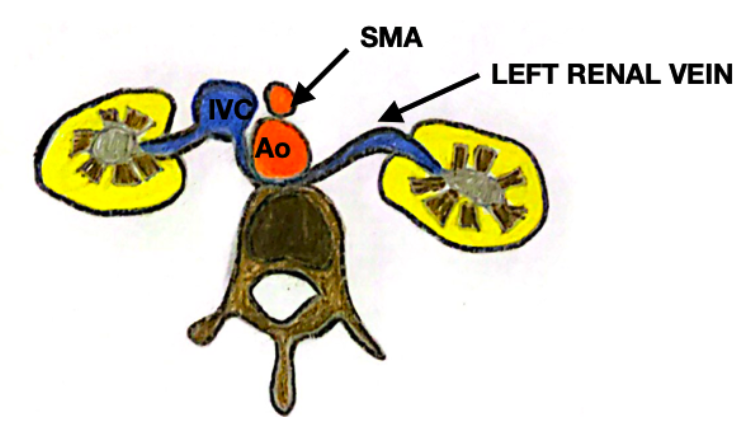
Figure 1. Schematic representation of posterior Nutcracker syndrome. SMA= Superior mesenteric artery; Ao= aorta, IVC= inferior vena cava.
Figure 2. Schematic representation of anterior Nutcracker syndrome. SMA= Superior mesenteric artery; Ao= aorta.
Figure 3. Schematic representation of May-Thurner syndrome.
Figure 4. Retro-aortic left renal vein (green arrow).
Figure 5. Dilatation of parauterine veins (green line)
Figure 6. ROV insufficiency (green line).
PVCS is a challenging diagnosis, due to aspecific symptoms and lack of globally accepted diagnostic algorithms and it is therefore under-diagnosed and poorly managed from a therapeutic perspective.