PRACTICAL GUIDE TO PERFORM AND REPORT AN WB-DW-MRI STUDY FOR CARCINOMATOSIS OF GYNECOLOGICAL ORIGIN
PRACTICAL GUIDE TO PERFORM AND REPORT AN WB-DW-MRI STUDY FOR CARCINOMATOSIS OF GYNECOLOGICAL ORIGIN
Ana García Bolado, Javier García Prado, David Castanedo, Carmen González-Carreró Sixto.
The aim of this work is to create a practical and complete guide so that any radiologist not used to performing WB-DW-MRI studies for carcinomatosis of gynecological origin can carry out a study of good diagnostic quality as well as an exhaustive report with the certainty that the report will cover allimportant features that other specialists involved in the carcinomatosis process (oncologists, surgeons, gynecologists...) need to know in order to decide the most appropriate treatment for the patient.
The objective of this study is to ASSESS IF THERE IS ANY CRITERIA THAT PREVENTS COMPLETE CYTOREREDUCTION (R0) to select women candidates for surgery. MRI - DWI of the whole body is useful to quantify and describe the tumor load prior to surgery and predict success in complete cytoreduction. There is a significant correlation between the extension of the disease in MRI - DWI of the whole body and surgery. Imaging protocols There are several suitable protocols for this study, as long as they include DWI sequences and IV contrast. We recommend performing an RMDWICE study that also includes the thorax, to also assess the existence of extra-abdominal disease, mainly pleural involvement, axillary and pericardiophrenic lymph nodes (they could go unnoticed with an exclusively abdominal study, even if completed with a thoracoabdominopelvic CT). We propose the protocol used by Garcia Prado J and Michielsen, cited in the bibliography, which includes axial and coronal sequences enhanced on T2, DWI and T1 fat saturation after gadolinium administration. Image processing Images can be examined both in the sequences obtained or after processing. Processing includes obtaining MIP reconstructions as well as fusion of different sequences; the most useful are those combining T2 and DWI sequences and as well as T2 combined with contrast-enhanced images, since they provide a precise anatomical localization of the DWI-restricting or contrast-enhancing implants. This fusion is performed both in the axial and coronal planes and gives a very visual idea, both morphological and functional, of the extent of the disease, which is very useful for displaying the images in the Gynecological Tumors Committee Structured report We propose a report in which, for greater clarity, the following is detailed separately: -Pelvic disease: ovarian masses, extension to pelvic organs, pelvic peritoneum and its recesses, pelvic lymph node involvement, ascites -Lower hemiabdomen disease: Related implants with ID loops, colon, mesentery root, infrarenal lymph nodes, ascites -Upper hemiabdomen disease: subphrenic, perihepatic and perisplenic implants, lymph nodes above the renal hilum, omental pie, ascites -Extra-abdominal disease: mediastinum, lymph nodes, pleuropulmonary involvementComplications that contraindicate or make surgery difficult, such as intestinal or urinary obstruction - Other findings not related to the extent of the disease
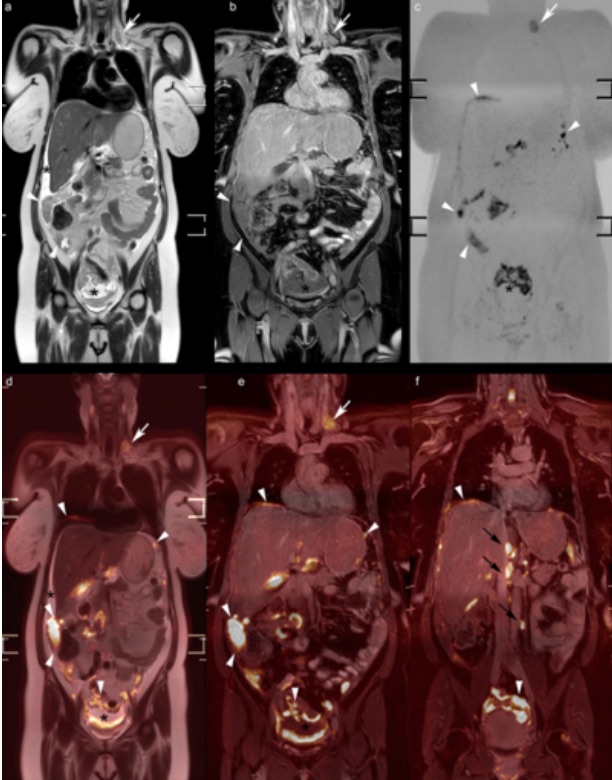
Coronal images T2WI, T1WIGad and DWI (top row) as well as merged with each other (bottom row), showing the advantages of combining anatomical location and behavior in DWI and after contrast to assess both the location and extent of tumor implants
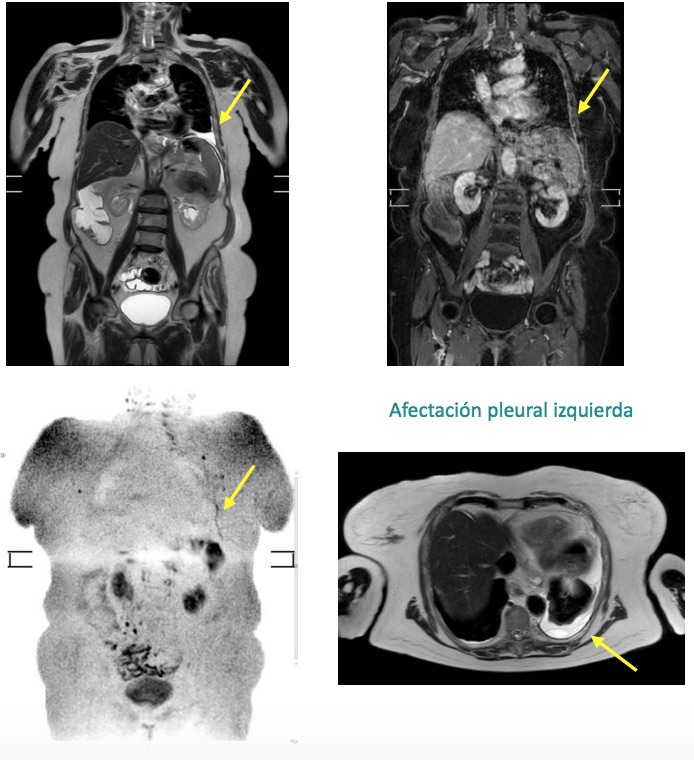
Another example of the different sequences included in the proposed protocol and how the combination of sequences provides both anatomical and functional information on the spread of the disease extending, in this case, to the thorax.
Subphrenic implants
Implants in Morrison peritoneum and falciform ligament
Nodular enhancement on DWI of the transverse colon wall suggestive of parietal implants
Implants in mesocolon of the splenic flexure of the colon in axial T2WI and DWI
Left pleural involvement
WBDWMRI study for the extension of peritoneal carcinomatosis of gynecological origin is complex and requires an exhaustive review of the images. Following the indications proposed in this work, it is possible, even for a radiologist not experienced in this technique, to make an accurate report that contains adequate and sufficient information to make the best therapeutic decision in patients with ovarian carcinoma in advanced stages.