Evaluation of extraprostatic neoplastic extension through Multiparametric Magnetic Resonance of the Prostate.
Evaluation of extraprostatic neoplastic extension through Multiparametric Magnetic Resonance of the Prostate.
Ariane Giovanaz Alice Schuch , Carmen Estivallet , Ivan Morzoletto Pedrollo, Rubia Vanceta
The aim of this study is to evaluate the accuracy of preoperative multiparametric prostate magnetic resonance imaging (mpMRI) in detecting extra-prostatic extension (EEP) of prostate cancer (PCa) using the Mehralivand scale, in comparison with the anatomopathology of the surgical specimen (gold standard).
PCa is extremely important clinically, being the second most common tumor in men and causing high morbidity and mortality rates. Local staging is responsible for risk stratification, which also includes free PSA, PSA density and Gleason score. For local staging, it is necessary to assess the EEP, which can be characterized as focal ( 1mm). Non-focal EEP characterizes a T3 tumour, which correlates with a high risk of positive surgical margins, metastatic disease, biochemical recurrence and low survival rates after radical prostatectomy. The mpMRI is already a well-established and widely used method for the detection of clinically significant tumors (Gleason >= 7), localization and characterization of lesions, biopsy with image fusion, control in active surveillance, recurrence evaluation, as well as for the planning of focal therapy and radiation. However, most of the current literature reports that mpMRI shows low sensitivity and only moderate specificity in assessing extraprostatic extension, especially when assessed by inexperienced radiologists. More recent studies have shown that the application of a system for predicting extraprostatic extension, using more objective criteria, such as the extent of curvilinear contact, capsular irregularity and bulging, asymmetry of the vasculonervous bundles, even the frank invasion of the periprostatic fat and seminal vesicles, have proved to be more accurate than the use of binary terms as in the case of absent or present extraprostatic extension. In our daily practice, we use the Mehralivand EEP prediction scale, which uses objective criteria and has four distinct categories: being grade 0 contact or = 1.5 cm or bulging/irregularity of the prostatic contour; grade 2 contact > or = 1.5 cm and bulging/irregularity of the external prostatic contour; and grade 3 frank measurable extension. Methods: This was a single-center, cross-sectional study, with retrospective collection of objective data and EEP scale reported in the preoperative mpMRI report and data from the surgical specimen AP of 105 patients who underwent radical prostatectomy and had mpMRI available in a digital file between April 2021 and August 2022. The mpMRI images and anatomopathological data for each patient were reviewed simultaneously. In mpMRI, EEP was considered according to the classification previously provided in the study reports, according to the Mehralivand criteria. The mpMRI scans were performed on 1.5 and 3.0 Tesla devices, following the PI- RADS v 2.1 protocol and interpreted by 07 abdominal radiologists with experience in mpMRI evaluation. All surgical procedures were performed in a tertiary hospital, using laparoscopic or robotic surgery. The AP was analyzed according to the report provided at the time of the examination, with absent extension, focal present and non-focal present. The surgical specimens were evaluated by 02 pathologists with experience in PCa. Chi-squared and ANOVA tests were used to detect differences among groups. Agreement between mpMRI image and the histology findings in the same patient was assessed using the kappa coefficient and percentage of agreement. The significance level adopted was 5%.
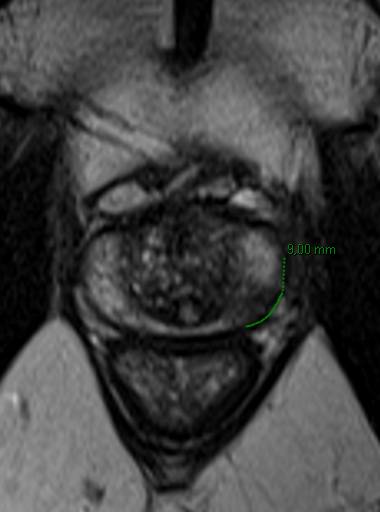
Focal alteration in the posterolateral peripheral zone of the middle third of the left lobe of the prostate, characterized as PI-RADS 4, showing contact with the external contour of the prostate for about 0.9 cm, without bulging or irregularity (EEP-MRI scale grade 0). AP did not show EEP
Focal alteration in the anterior transition zone of the right lobe of the prostate, characterized as PI-RADS 4, presenting a small area of contact with the anterior prostatic contour (around 0.8 cm), with slight bulging of the external prostatic contour (grade 1 suspicion for EEP by MRI). AP did not show EEP
Elongated focal lesion in the posteromedial/lateral peripheral zone of the middle third to the base of the right lobe of the prostate, characterized as PI-RADS 4, presenting contact with the external contour of the prostate for about 2.2 cm, with irregularity of the prostatic contour, characterizing EEP grade 2 by MRI.AP confirmed EEP
Most of the lesions were classified as grade 0 EEP on mpMRI (52, totaling 49.5% of the sample), 22 lesions were classified as grade 1 and 2 EEP respectively, making up 21% of the sample and 09 lesions were classified as grade 3 EEP, totaling 8.6% of the sample. In the AP analysis of the surgical specimens (gold standard), 72 patients (68.6%) had no EEP, 13 (12.4%) had focal present EEP and 20 (19.0%) had non-focal present EEP. Among the 52 patients classified as EEP by mpMRI grade 0, 46 (88.5 %) did not show EEP in the AP, only 06 showed focal EEP (1 mm). Of the 09 patients classified as EEP by mpMRI grade3I, 8 (88.9%) confirmed non-focal EEP in the surgical specimen, and 01 patient did not show EEP (the patient did not have free surgical margins and did not have zero PSA figures after PR). However, patients classified as grade 1 (22 patients) and grade 2 (22 patients) EEP by mpMRI showed more heterogeneous results. Among those classified as grade 1, 15 patients had neoplasia confined to the prostate, 01 patient showed focal EEP and 06 patients showed non-focal EEP, while among those classified as grade 2, 10 patients did not have EEP, 05 patients showed focal EEP and 07 patients showed non-focal EEP. EEP detection rates ranged from 27.3% in patients classified as grade 1, 54.5% in patients classified as grade 2 and 88.8% in patients classified as grade 2. When we consider patients classified as having an EEP greater than or equal to 2 as positive, we see an accuracy of 77.1%, with a Kappa value of 46.1% (denoting moderate agreement) and 95% CI, sensitivity of 60.6%, specificity of 84.7%, positive predictive value of 64.5% and negative predictive value of 82.4%.
Focal alteration in the peripheral zone of the extreme apex of the left lobe of the prostate, characterized as (PI-RADS 4, in wide contact with the prostatic contour (>1.6 cm), with irregularity of the external contour, classified as EEP by MRI grade 2.
Macroscopy and pathology showed a tumor with extraprostatic extension at the apex of the left lobe.
ROC curve, which represents the ratio between observations classified as true positives (sensitivity) and false positives (1-specificity). The AUC result was 0.7266, i.e. the classification accuracy is 73%.
The Mehralivand EEP scale showed moderate accuracy in the preoperative assessment of EEP, with greater effectiveness at its extremes, and a good correlation between grade 0 and absence of non-focal extension and grade 3 and presence of non-focal extension. Grades 1 and 2 showed variability in results and can be considered indeterminate. Other characteristics, such as the extent of contact between the lesion and the external contour of the prostate, late enhancement of the adjacent capsule to the lesion and ADC map figures can be useful in assessing extraprostatic extension. Our study showed similar results to those found in the literature with an accuracy of 0.77 for detecting EEP, with a Kappa value of 46.0 %, denoting moderate agreement and a CI of 95 %.
An extensive bilateral prostate lesion, with an epicentre in the peripheral zone and the largest component located in the right lobe, extending from the base to the apex, with extension to the central zone and transition in its upper segment, characterized as PI-RADS 5, with signs of measurable EEP, classified as grade 3.
Macroscopy and anatomopathology showed a tumor with extraprostatic extension throughout the right lobe.