Soothing the headache of pregnancy and post-partum neurological complications: A pictorial review
Soothing the headache of pregnancy and post-partum neurological complications: A pictorial review
Amreen Shakur, Anne Buckley, Brooke Lawson, Janice Lee, Janette Smith, Ishwariya Rajendran, Helen Addley, Justin Cross, Tomasz Matys, Francis Scott and Sue Freeman
1.Increase in overall age of pregnancy has led to a consequent increase in pregnancy associated complications, which the radiologist should be aware of. 2.The complications can include exacerbations of pre-existing conditions, pregnancy-specific disorders as well as complications related to the delivery process. 3.We will illustrate common and more unusual neurological conditions which can occur in pregnancy and the post-partum period on CT and MRI.
Introduction Neurological complications in pregnancy and the post-partum period can lead to severe consequences for both the mother and child and can be challenging to diagnose due to relatively non-specific symptoms. Headache is a common symptom and experienced by up to 35% of pregnant women, however underlying causes can range from relatively innocuous migraines, to rare potentially life threatening conditions [1] . The general radiologist should be well-versed in potential conditions that may arise in this period to allow timely management. Due to availability, CT head is often the initial imaging study of choice and can readily detect acute haemorrhage and brain herniation syndromes. MRI has greater sensitivity, however, is more prone to artefact, requires more extensive safety checks and is less readily available in the out-of hours setting. It is also limited in that MRI is avoided within the first trimester of pregnancy and gadolinium based contrast imaging is not recommended at any stage of pregnancy unless absolutely necessary due it crossing the placenta and being associated with an increased risk of still birth and neonatal death [2][3] . Our review highlights the radiological appearances of common neurological complications which are cerebrovascular in nature as well as endocrine/metabolic complications. We also illustrate the appearances of common primary CNS conditions which can manifest during pregnancy and the post-partum period. Cerebrovascular Subarachnoid haemorrhage (SAH) The commonest cause of SAH is rupture of intracranial aneurysm and is associated with significant pregnancy-associated maternal and neonatal morbidity and mortality. Some studies have reported an increased incidence of SAH in pregnancy which likely relates to associated physiological changes which can increase the risk of intracranial aneurysm formation, growth, and rupture [4][5] . In 10% to 20% of all cases of SAH, no underlying vascular aetiology is found. Peri-mesencephalic SAH is a subset of non-aneurysmal SAH and is typically associated with a benign clinical course, excellent prognosis, and a low risk of rebleeding or other complications compared with aneurysmal SAH [6] . Venous sinus thrombosis (VST) and venous infarct/haemorrhage The hypercoagulable state of pregnancy, venous stasis and endothelial damage that can occur during labour and delivery increases the risk of thromboembolism in this period [7] . The highest incidence of VST is within the first two weeks post-delivery and clinical presentation varies from headache to loss of consciousness dependent upon the extent of thrombosis. Unenhanced CT is less sensitive however may demonstrate increased density (usually >70HU) within the dural venous sinuses. The venous outflow obstruction may result in venous hemorrhagic infarctions which are typically cortical or paramedian in location and not confined to a single arterial vascular territory [8][9] . CT venogram demonstrates filling defects within the venous sinuses. (Figure 1). MRI can show areas of parenchymal oedema and shows greater sensitivity in identifying microhaemorrhages. Acute ischaemic stroke/parenchymal haemorrhage There is an increased risk for ischaemic and haemorrhagic stroke of up to three-fold in pregnancy and the post-partum period, with the highest risk reported from the third trimester until six weeks post-partum [10] . Hypertensive disorders and hypercoagulability are thought to be key factors conferring the increased risk. The imaging features are similar to those seen in non-pregnant patients, with CT being relatively non-specific in the setting of acute ischaemic stroke. Typical features on CT include subtle loss of grey-white matter differentiation and hyperdense vessels representing acute thrombus. CT angiography (CTA) has a high sensitivity and specificity for identifying large vessel occlusion. CT perfusion is a useful adjunct to CT/CTA to identify regions of salvageable ischaemic brain tissue by assessing perfusion parameters (time to peak, cerebral blood flow and cerebral blood volume) which can guide subsequent management. The infarct core describes the region of ischaemia destined to infarct regardless of therapy and usually demonstrates prolonged time parameters with reduced cerebral blood flow and volume. Salvageable brain tissue surrounding the infarct core (ischaemic penumbra) can demonstrate prolonged time parameters with relatively normal cerebral blood flow and volume (Figure 2). MRI has greater sensitivity in the acute phase, where foci of diffusion restriction may be seen within minutes of the onset of stroke [10] . Pre-eclampsia/eclamptic encephalopathy Preeclampsia is a disorder of pregnancy associated with gestational hypertension and end-organ dysfunction. It affects approximately 6-8% of pregnancies and generally occurs after the 20 th week of pregnancy. Eclampsia is defined as the addition of new onset seizures and/or coma during in the setting of preeclampsia and occurs in up to 5% of pregnancies and is the second leading cause of maternal death after pulmonary embolism [11] . Typical MRI findings in eclampsia include vasogenic oedema with increased T2 signal in the posterior subcortical and deep white matter. These findings are also characteristic of posterior reversible encephalopathy syndrome (PRES) suggesting a common pathophysiology. Less common features are that of postpartum angiopathy with segmental vasoconstriction which can also manifest as ischaemia with cytotoxic oedema or haemorrhage. Posterior reversible encephalopathy syndrome (PRES) Posterior reversible encephalopathy syndrome typically evolves over a matter of hours and presents with rapid onset of symptoms including headache, seizures, altered consciousness, and visual disturbance. Predisposing factors include hypertension and pre-eclampsia/eclampsia. Although the underlying mechanism is unclear, endothelial dysfunction and interruptions in brain auto-regulation are thought to be important factors [12] . Typical MRI findings include symmetric white matter oedema in vascular watershed areas in the posterior regions of both cerebral hemispheres, affecting mostly the occipital and parietal lobes. Atypical features including white matter oedema in mid and posterior aspects of the superior frontal sulcus, asymmetrical changes with isolated involvement of the frontal lobes, inferior temporo-occipital junction, basal ganglia and cerebellum. Three main patterns of haemorrhage associated with PRES have been described including focal parenchymal haemorrhage, microhaemorrhages and subarachnoid haemorrhage. (Figure 3) Reversible cerebral vasoconstriction syndrome (RCVS) RCVS encompasses a group of entities characterized by recurrent thunderclap headaches and reversible multifocal cerebral vasoconstrictions. The pathophysiology of this syndrome remains unknown; however, disturbance in cerebral vascular tone and consequent vasoconstriction are thought to be key factors. [13] The key imaging feature of RCVS is arterial vasoconstriction involving multiple vascular territories of medium to large cerebral arteries, with multi-focal areas of arterial narrowing interspersed with normal calibre segments, visualised as a “string of beads” [14] . Digital subtraction angiography (DSA) has a greater sensitivity than CTA or MRA, however neuroimaging is often reported as normal at the onset of symptoms. Early MRI features of cortical oedema and both sulcal and cortical foci of increased signal on FLAIR imaging have been described which may precede the onset of vasoconstriction [15] . (Figure 4.) There can be overlap of imaging features in RCVS and primary angiitis of the CNS (PACNS), however some distinguishing features have been reported. Whilst initial imaging in RCVS is normal, approximately 90% of patients with vasculitis show multifocal infarcts of varying ages. Haemorrhagic complications are more commonly seen in RCVS, with subarachnoid haemorrhage encountered more frequently than intraparenchymal haemorrhage. Some studies have shown techniques such as vascular wall imaging MRI to be a useful adjunct which demonstrate contrast enhancement to be more intense in PACNS as compared to RCVS [16] . Metabolic Pituitary apoplexy/Sheehan’s syndrome Pituitary apoplexy describes a clinical syndrome related to haemorrhagic infarction of the pituitary gland, usually in the context of a pre-existing macroadenoma. The commonest symptom is of sudden headache that is frequently retro-orbital in location [17] . Sheehan syndrome specifically refers to the haemorrhagic necrosis within the anterior pituitary gland following significant post-partum bleeding, hypovolemia, and shock [18] . As well as headache, patients may present with pan- hypopituitarism. The underlying pathophysiology in pregnancy is thought to relate to hyperplasia of the prolactin-producing cells due to elevated oestrogen levels resulting in gland enlargement. This in turn can cause secondary compression of the blood vessels supplying the anterior pituitary gland. The anterior pituitary gland is a relatively low- pressure system, making it more susceptible to ischaemia and therefore more prone to necrosis in pregnancies complicated by significant intrapartum and post-partum haemorrhage. Typical MRI features in the acute phase is that of an enlarged pituitary, sometimes with a fluid level with associated mass effect on the surrounding structures. Signal intensity changes on T1 and T2 weighted sequences are based on the stage of haemorrhage [19] . SWI may show blooming artefact. Dural thickening and thickening of the sphenoid sinus mucosa has also been described. After several weeks, the pituitary gland may become atrophied leading to an ‘empty sella’ appearance. (Figure 5) Lymphocytic hypophysitis Lymphocytic hypophysitis is the most common type of primary hypophysitis and is characterised by a non-neoplastic infiltration into pituitary gland causing its dysfunction, secondary to autoimmune mechanisms. Typical MRI features include pituitary gland enlargement, loss of the posterior pituitary bright spot, infundibular thickening with adjacent dural/sphenoid sinus enhancement. Primary CNS conditions manifesting in pregnancy. Primary brain malignancies The hormonal changes that occur during pregnancy were previously believed to increase the detection rate of certain tumours including meningiomas, however this has not been substantiated in recent studies [20] . In patients with prior or current history of known high grade tumours, a link between pregnancy and tumour progression has been shown [21] . (Figure 6, 7.) Multiple sclerosis (MS) Several studies have investigated the effects of pregnancy on multiple sclerosis and have demonstrated a lower rate of MS relapse, particularly in the third trimester which is likely due to the immunotolerant state of pregnancy [22] . However the risk of relapse has been reported to increase in the post-partum period of up to three-fold compared to that of baseline [22] . (Figure 8.)
26 year-old female, 3 weeks post-partum (induced vaginal delivery) experiencing a 3-day history of migraine, presented to the emergency department with multiple seizures, urinary incontinence and a GCS of 3. (a) Unenhanced CT in axial, (b) sagittal and (c) coronal reformats demonstrated hyperdensity within the superior sagittal sinus (red arrows). CT venogram in (d) axial, (e) sagittal and (f) coronal reformat confirms filling defects within the left transverse and superior sagittal sinuses (red arrowheads) extending into the sigmoid and left internal jugular veins (not shown) in keeping with extensive venous sinus thrombosis.
27 year old, 7 week pregnant female presented to ED with sudden onset of left sided headache, slurred speech and right sided weakness. (a) Unenhanced CT demonstrated a subtle hyperdensity in the region of the left MCA (red arrow). (b) Reconstructed CT-angiogram images demonstrated a corresponding filling defect within the M2 segment of the left MCA (white arrow).(c) Time to perfusion and (d) corresponding lesion MAP from CT perfusion study demonstrated increased time parameters (arrowheads), with no corresponding reduction in cerebral blood flow or blood volume (not shown). Overall features consistent with hyperacute left MCA infarct with a reasonable ischaemic penumbra. Patient subsequently underwent thrombolysis and made a full recovery.
41 year old female, 23 weeks pregnant with a history of multiple miscarriages presented to ED with acute confusion and thrombocytopenia. Unenhanced axial CT (a) demonstrated a subtle focus of vasogenic oedema within the right frontal lobe (red arrow). (b) axial CTA demonstrated subtle focal narrowing within the left anterior cerebral artery (red arrowhead) (c) axial FLAIR images demonstrated increased signal intensity extending to the cortical U-fibers (blue arrow) and patchy increased signal within the deep white matter (blue arrowhead). (d,e) DWI demonstrate multiple foci of diffusion restriction consistent with acute infarcts (green arrows). (f) SWI also demonstrated multiple foci of microhaemorrhage (green arrowhead) The multiple acute infarcts and several old infarcts and foci of haemorrhage are consistent with thrombotic microangiopathy in keeping with the patient’s known history of thrombotic thrombocytopenic purpura, however a differential diagnosis of RCVS was considered at the time. Focal vasogenic oedema within the right frontal lobe is consistent with PRES.
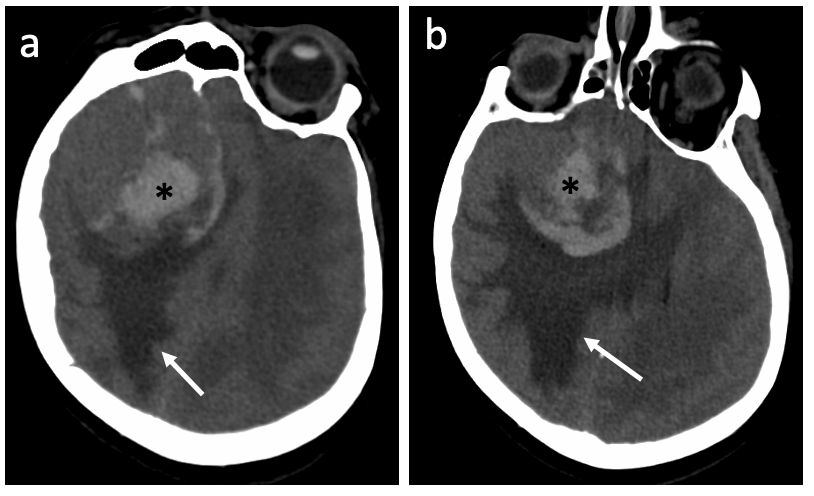
37 year old female experienced severe headache and left hemiplegia while being induced for labour. (a) Unenhanced axial CT demonstrates large volume intraparenchymal haemorrhage (asterisk) in the right frontal lobe with surrounding oedema and subfalcine herniation and intraventricular haemorrhage within the frontal horn of the right lateral ventricle (arrowhead) and third ventricles. Small volume subarachnoid haemorrhage in the cortical sulci was also present (not shown). (b) Maximum intensity projections (MIP) from CTA images demonstrate segments of subtle arterial narrowing in the anterior cerebral artery (red arrows). (c) Digital subtraction angiography images demonstrate more conspicuous segments of luminal narrowing (red arrows) in the right anterior circulation alternating with normal calibre vessel giving a beaded ‘string of pearls’ appearance consistent with RCVS.
33-year old female experienced significant post-partum haemorrhage of 1.5L and lost consciousness. Initial CT head was normal and subsequent MRI was performed. (a) Sagittal T1 and (b) coronal images demonstrated a mildly enlarged pituitary gland with a focus of internal high signal (arrow) within the anterior pituitary gland in keeping with haemorrhage. Following the initial acute event, the patient experienced pan-hypopituitarism and subsequent MRI three months later (c,d) demonstrated a small residual anterior pituitary gland (arrowhead)
33 year old female, 36 weeks pregnant presented with headache.(a)(b) Unenhanced axial CT demonstrated a large extra-axial lesion within the right frontal lobe with internal haemorrhage (asterix) and significant surrounding vasogenic oedema (white arrow) and subfalcine haemorrhage. Overall features are consistent with a meningioma with internal haemorrhage.
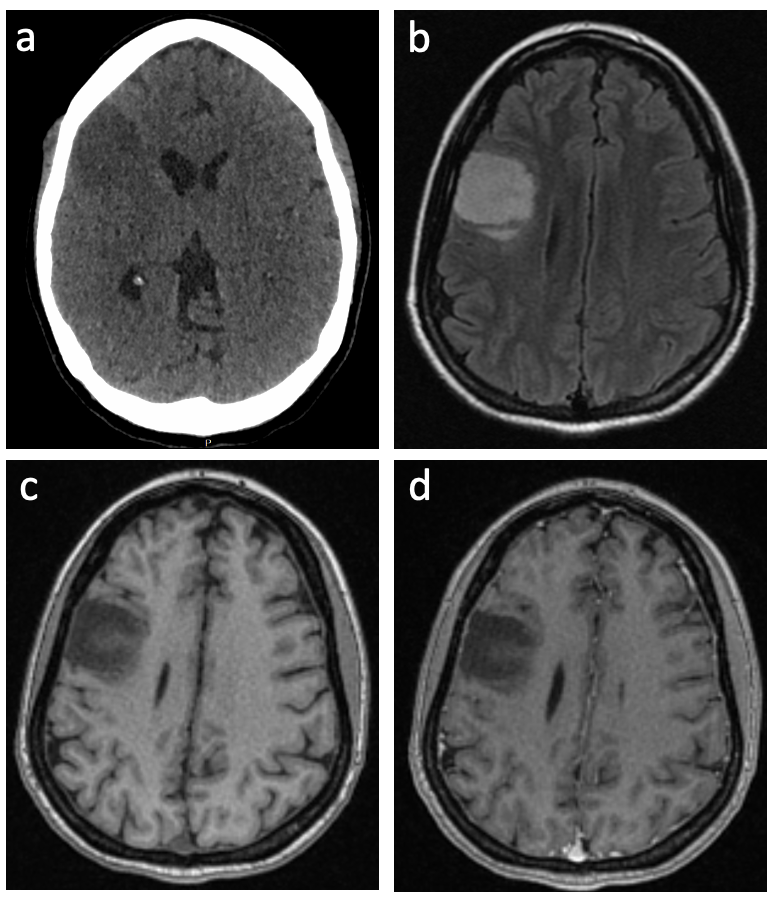
35 year old female, 24 weeks pregnant presented with collapse, seizure and loss of consciousness. (a) Unenhanced CT demonstrated a region of hypodensity within the right frontal lobe. Subsequent MRI for further characterisation revealed this lesion to be of high signal on FLAIR (b), low signal on T1WI (c) with no evidence of post contrast enhancement (d). Overall features consistent with a low-grade glioma and subsequent histology confirmed diffuse astrocytoma.
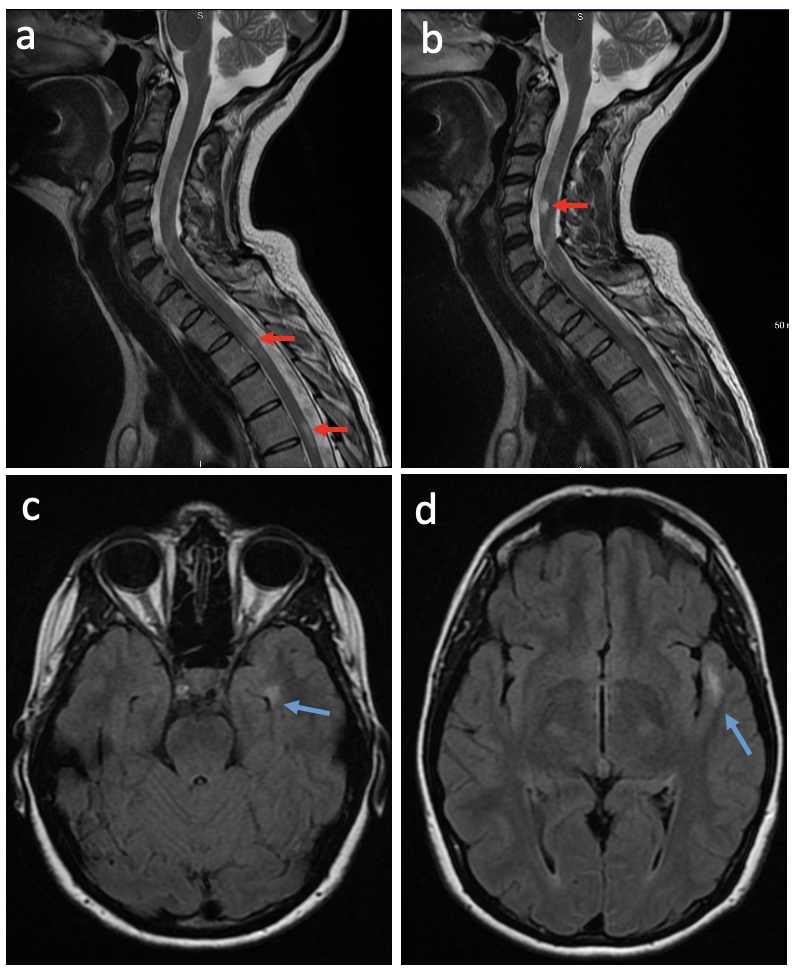
32 year old, 17 week pregnant patient presented with right foot paresthesia. (a,b) Sagittal T2 sequences from initial non-contrast MRI of the spine demonstrated several short segment lesions of increased signal intensity within the cervical and thoracic spine (red arrows) suspicious for demyelination. (c,d) Axial FLAIR sequences demonstrate high signal intensity lesions within the left temporal lobe (blue arrows). Subsequent postnatal MRI with contrast revealed multiple new lesions with varying levels of contrast enhancement. Overall findings consistent with multiple sclerosis.
Neurological complications in pregnancy and the post-partum period pose a diagnostic challenge due to non-specific symptoms which encompass a spectrum of benign and life-threatening conditions. Knowledge of the key radiological findings in conditions encountered during this crucial period is essential to ensure prompt diagnosis and management.