mp-MRI appearance of primary and secondary prostate lymphomas
mp-MRI appearance of primary and secondary prostate lymphomas
Patricia GUTIERREZ, Mickael LAIR, Philippe PUECH
-To present the most common lymphoid affections of the prostate. -To describe the different appearances of primary and secondary prostate lymphomas at prostate mp-MRI. -To summarize the clinical presentations and differenciate them with prostate adenocarcinoma.
Lymphomatous involvement of the prostate is rare, accounting for only 0.09% of all prostate neoplasms. It can manifest as either a primary prostate lymphoma (PPL) or, more commonly, as a secondary involvement (SPL) occurring in 0.1% of all Non Hodgkin Lymphomas (NHL). Prognosis is usually poor. Prostate lymphoma has a bimodal clinical distribution: PPL is more frequently seen in elderly patients, with a mean age of 62 years, while SPL occurs in younger patients.[1,2,3] The main criteria to define PPL involvement proposed by Bostwick and Mann consist in: 1) symptoms attributable to prostatic enlargement, 2) the prostate as the predominant site of involvement, and 3) the absence of involvement of liver, spleen, or lymph nodes within one month of diagnosis. [4] Prostate lymphoma usually presents as lower urinary tract obstruction that does not respond to symptomatic medication. Compared to other prostatic obstructive diseases, it tends to progress rapidly and may show only a slight or no increase in PSA levels. A history of lymphoid disease, systemic symptoms such as fever, chills, night sweats, weight loss, or peripheral adenopathies can suggest the diagnosis.[5] Transrectal ultrasound (TRUS) of the prostate reveals an enlarged gland and a prostate mass, prompting the need for Multiparametric prostate MRI (mp-MRI). mp-MRI accurately describes the lesions and their potential extension to the surrounding structures (seminal vesicles, periprostatic fat). It also helps differentiate from aggressive prostate adenocarcinoma, sarcoma, and other rare prostate tumors. A diagnosis by prostate biopsy is mandatory to initiate chemotherapy.[2] Results: ====== We will describe three types of lymphomatous prostate gland involvement, and their semiology at mp-MRI (fig 1) : a) Localized nodular type ; b) Extensive tissular mass (sarcoma-like) and c) Periprostatic and periseminal involvement. Localized nodular type: (fig 2, 3) --------------------------- Lymphoma with a nodular pattern involving only the prostate gland is infrequent. It can be related to follicular subtype, Mantle cell and Burkitt lymphomas, although it can also be an early form of diffuse large B-cell lymphoma (DLBCL), the most frequent subtype. As clinically they can be indolent, they don’t cause PSA elevation and they can be missed in digital rectal examination, most of these are diagnosed on LUTS material or at MRI due to PSA elevation for concomitant inflammation or synchronously to a prostate adenocarcinoma. [6] At MRI, ther can be a single or multiples nodules, appearing iso - hypointense on T2WI, localized to the gland without causing loss of the regional differentiation or extraprostatic extension. On DWI there is an important restriction due to the hypercellularity and in DCE they are hypovascularized. Involvement of the transition zone often causes misdiagnosis and difficulties in giving a PIRADS score. Extensive tissular intraprostatic mass: (fig 4) --------------------------------------------- This is the most frequent presentation, and in most cases this presentation is related to DLBCL. It is an aggressive form, that usually comes with urinary symptoms such as acute urinary retention. [7] The prostate volume is increased but with relative conservation of its shape (this is why some authors refers to it as “prostatomegaly”). Infiltration is heterogeneously iso-hypointense on T2WI but isointense on T1WI and invades almost the whole parenchyma. [8] On DWI there is an important restriction but no clear enhancement. There can be some areas of necrosis and cystic degeneration. [9] Periprostatic and periseminal involvement: (fig 5, 6) ------------------------------------------------- This type is exceptional, usually reported as SPL and it can be associated with immunosuppression. The cellular types involved in the literature include follicular lymphoma, Burkitt lymphoma and intravascular large B-cell lymphoma. [4] There is an infiltration of the peri prostatic and seminal fat, with encompassement of vascular and nervous structures. This tissue has the same characteristics as other forms : mildly low signal intensity on T2WI, restriction on DWI/ADC because of the cellularity, and slow enhancement (hypovascularized). Key points to differentiate PL from adenocarcinoma (PCa): (table 1) -------------------------------------------------------------------- Patients with PL are usually symptomatic, presenting urgency, frequency, painful urination, hematuria, increased nocturia, dysuria, and acute urinary retention, while specific symptoms associated with lymphoma such as fever, night sweats, and weight are not frequent in early stages.[2] PSA value is generally normal or low in PL in comparison with PCa.[10] T2 signal is intermediate, very homogeneous, lesion shows very low ADC, and enhancement is weak, whereas T2WI signal is usually very low, restriction is variable and enhancement is strong and early in case of PCa.
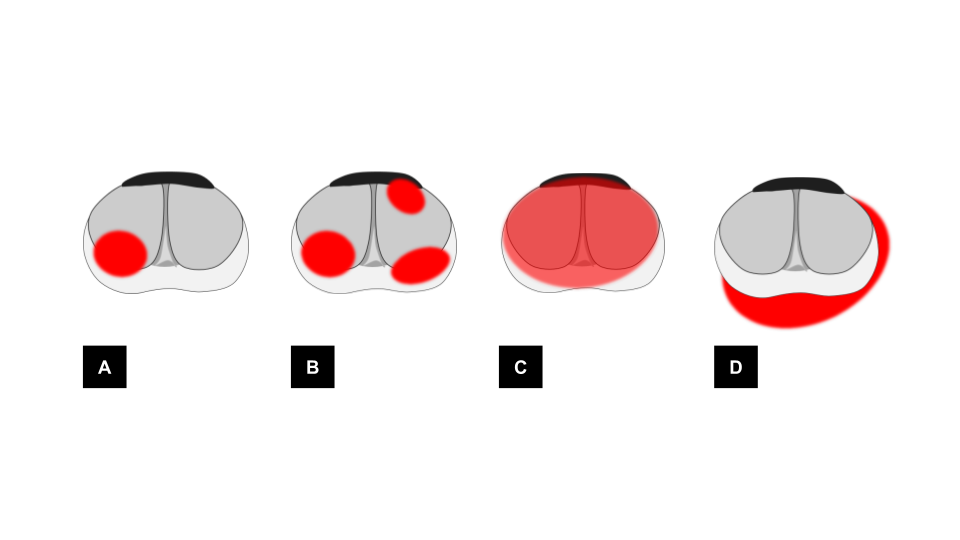
Fig 1. Illustration of the 3 main prostate lymphoma involvement patterns. A. localized nodular type (unique) ; B. localized nodular type (multiple) ; C. Extensive tissular intraprostatic mass ; D. Periprostatic and periseminal involvement
Fig 2. Localized nodular type (unique). A. axial T2WI intermediate signal nodule of the anterior and medial transition zone of the prostate base (arrow) ; iliac extern adenomegalies (dotted arrow) B. sagittal T2WI the nodule is in the intravesical protrusion (arrow). C. DWI b 2000 / ADC shows strong restriction of the nodule (arrow) and the lymph nodes. D. axial T1WI early phase E. axial T1WI FS late phase F. axial T1WI FS late phase shows progressive heterogeneous enhancement (arrow). Pathology revealed a small B cell lymphoma.
Fig 3. Localized nodular type (multiple). A. axial T2WI shows three nodules of intermediate signal at the basal peripheral zone (arrows) B. coronal T2WI. C. DWI b 2000 / ADC shows strong restriction of the nodules. D. axial T1WI before contrast, and E. at early phase shows homogeneous and hypervascularization. F. Doppler US showed hypoechoic and Doppler positive masses in the gland before biopsies. G. FDG-PET-CT demonstrated multiple other localizations. Pathology revealed a MALT type extranodal marginal zone B-cell lymphoma.
Fig 4. Extensive tissular intraprostatic mass. A. Coronal T2WI homogeneous infiltration of the whole prostate with intermediate signal (arrow) B. axial T2WI periprostatic and perirectal extension (arrow) C. Coronal T2WI (zoom) involvement of the right seminal vesicle and prostate - bladder angle (arrow). D. and E. DWI B1600 and ADC map show restriction F. DCE shows low to moderate homogeneous enhancement. The biopsy revealed a large B cell lymphoma.
Fig 5. Periprostatic and periseminal involvement. A. B. Axial T2WI of the base of the prostate and seminals shows an homogeneous infiltration of the periprostatic space, seminal and bladder (arrow) C. coronal T2WI. This infiltration is homogeneous and isointense in T2WI (arrow) D. sagittal T2WI shows how this infiltration follows the direction of the peritoneal reflection up to the perirectal space (arrow). E. and F. DWI B2000 and ADC map show deep restriction. G and H. DCE shows low to moderate homogeneous enhancement. I. and J. PET - CT FDG axial ; shows captation of periprostatic tissue and also reveals bone infiltration. The pathology was a Burkitt lymphoma.
There are three distinct presentations of prostatic lymphomas (PL), with their own patterns of spread and imaging characteristics. MRI is useful for the positive diagnosis, extension and follow-up, but also for differential diagnosis. Symptoms of urinary obstruction, low PSA level, and/or history of preexisting systemic lymphoma or immunosuppression are other relevant indicators to evoke PL instead of classic prostate adenocarcinoma. References ------------ 1. Han C, Zhu L, Liu X, Ma S, Liu Y, Wang X. Differential diagnosis of uncommon prostate diseases: combining mpMRI and clinical information. Insights Imaging. 2021;12: 79. 2. Ren M, Liu Y. Primary diffuse large B-cell lymphoma of the prostate: a case report and review of the literature. J Med Case Rep. 2021;15: 1–5. 3. Wang K, Wang N, Sun J, Fan Y, Chen L. Primary prostate lymphoma: A case report and literature review. Int J Immunopathol Pharmacol. 2019;33. doi:10.1177/2058738419863217 4. Primary non-metastatic extra-nodal diffuse large B-cell lymphoma of the prostate and seminal vesicle. Urology Case Reports. 2022;40: 101945. 5. Petrakis G, Koletsa T, Karavasilis V, Rallis G, Bobos M, Karkavelas G, et al. Primary prostatic lymphoma with components of both diffuse large B-cell lymphoma (DLBCL) and MALT lymphoma. Hippokratia. 2012;16: 86–89. 6. Website. doi:10.1002/(SICI)1097-0142(19980815)83:43.0.CO;2-T 7. Ab Hamid S. Primary Prostatic Lymphoma Presenting with Prostatomegaly. Radiol Imaging Cancer. 2023;5: e220171. 8. Monzen Y, Nakahara M, Nishisaka T. Spontaneous Regression of Primary Malignant Lymphoma of the Prostate. Case Rep Urol. 2013;2013. doi:10.1155/2013/363072 9. Nepal P, Nagar A, Tirumani SH, Ojili V. Imaging of non-epithelial neoplasms of the prostate. Abdominal Radiology. 2020;45: 4117–4132. 10. Follicular lymphoma presenting as a seminal vesicle mass: Diagnostic path from prostate MRI to 18F-FDG PET/CT. Radiology Case Reports. 2023;18: 2768–2770.
Fig 6. Periprostatic and periseminal involvement. A. B. C. Axial T2WI of the mid gland, base of the prostate and seminals shows an homogeneous infiltration of the periprostatic fat (arrow) D. E. DCE shows low to moderate homogeneous enhancement F. DWI B2000 and ADC map show strong restriction. G. PET - CT FDG, axial shows captation of periprostatic tissue. H. There was no other involvement in PET-CT. The pathology was a MALT type extranodal marginal zone B-cell lymphoma
Table 1: Imaging, biological and clinical features that help differentiate PL from adenocarcinoma.