Imaging in renal cell carcinoma – (a)typical findings
Imaging in renal cell carcinoma – (a)typical findings
Inês Dias, Raquel Dias
To review the relevant demographic, clinical and histologic features of renal cell carcinoma (RCC). To describe and illustrate the imaging features of histologic subtypes of RCC with cases from our institution. To identify the main list of differential diagnoses.
RCC constitutes 2%-3% of adult malignancies and is the most common adult epithelial cancer representing 90% of renal tumors (2, 3, 4). RCC can be familial or sporadic. Endogenous risk factors include older age (the median age at diagnosis is 65 years), male sex, having a first-degree relative with RCC and inherited genetic syndromes including von Hippel-Lindau disease, hereditary papillary renal cancer, Birt-Hogg-Dubé syndrome, tuberous sclerosis, which are associated with the development of several benign and malignant tumors in different organs (2, 5). Exogenous risk factors include lifestyle factors, such as smoking, obesity, hypertension, dietary factors, radiation exposure (2, 5). The incidence of RCC is increasing because of the increased use of abdominal imaging (4, 7). Most RCCs are asymptomatic and are incidentally detected (3). Over the last few decades the early diagnosis of RCCs is possible because of the wide availability of high-resolution cross-sectional imaging modalities. Therefore, these incidental RCCs are often detected at a smaller size and lower stage (4, 7). The classic triad of flank pain, visible haematuria and palpable abdominal mass is rare, occurring in only 6%-10% of patients and predicts a more aggressive histology, advanced disease and poor outcomes (2). The main histological subtypes of RCC are clear cell, papillary and chromophobe tumors accounting for 70%, 10%-15% and 5% of RCCs respectively, with different prognosis and response to treatment (3, 4). These subtypes have different imaging features that can be characterized by a multimodality imaging approach including the use of ultrasound (US), computed tomography (CT), magnetic resonance (MR) imaging and positron emission tomography (PET) (1, 4). The clear cell subtype of RCC is the most common variant and has the least favourable prognosis. Most clear cell renal carcinomas are sporadic (95%) and the remaining are associated with hereditary syndromes like von Hippel-Lindau disease (2, 6). Clear cell renal carcinomas originate from the renal cortex and present a predominantly expansile growth pattern (2, 6). Their imaging findings are in accordance to their histopathological features (hypervascularized and heterogeneous lesions due to necrosis, hemorrhage, cysts and calcifications) (5, 6, 7) (Figures 1, 2, 3). The papillary variant of RCC is associated with acquired chronic renal disease and presents with different imaging features. Papillary RCCs tend to be solid, well defined, slow growing lesions that can also be bilateral and / or multifocal (more prevalent than in other subtypes). At CT and MRI these tumors are typically homogeneous and hypovascular (Figure 4). Bigger lesions may be heterogeneous due to the presence of necrosis, hemorrhage and calcification. The presence of internal foci of macroscopic fat is extremely rare (5, 6, 7). The chromophobe subtype of RCC carries the best prognosis (6). Most of these tumors are sporadic and rare hereditary forms include Birt-Hogg-Dubé (2). They share histopathological and imaging features to oncocytomas (4, 7) (Figures 5, 6). They are more homogeneous than clear cell carcinomas and can exhibit a central scar (like oncocytomas) (5, 6, 7). Other less common subtypes include collecting duct carcinoma and medullary RCC (both with infiltrative patterns of growth and poor outcomes), multilocular cystic RCC (with excellent prognosis after nephrectomy) (2, 6). Imaging is also useful to detect local recurrence (Figure 7) and metastatic disease. About 33-50% of patients have metastatic disease at the time of diagnosis (Figure 8). Approximately 20-40% of patients with RCC develop metastatic disease after radical nephrectomy (8). RCC typically metastasizes to the lung, bone, lymph nodes, liver, adrenal glands (Figure 9) and the brain, with the lung being most frequently involved by clear cell tumors and the liver by chromophobe tumors (3, 8). Other than metastases, other signs in favor of malignancy are: invasion of the perinephric fat, extension to the renal vein or inferior vena cava (Figure 10), the presence of regional adenopathies and invasion of adjacent organs (1, 8). The main differential diagnoses include benign tumors like oncocytoma (that mimics RCC on imaging), angiomyolipoma; others malignant renal tumors (renal metastasis, renal lymphoma) and pseudotumors (complex cysts, abscess) (2, 3).
Figure 1 – Clear cell RCC in a 62-year-old male patient. The ultrasound shows a mass in right kidney with a heterogeneous and hypervascularized solid component and cystic areas.
Figure 2 – Clear cell RCC in a 62-year-old male patient. The CT imaging (axial pre-contrast (A), corticomedullary (B) and nephrographic (C) phases) shows an expansile heterogeneous lesion in right kidney with cystic areas and solid component with intense contrast uptake at the corticomedullary phase (120-140HU) and washout in the nephrographic phase (90-100HU).
Figure 3 – Clear cell RCC in a 66-year-old female patient. The MRI shows a nodule in the right kidney that is moderately hyperintense on T2-weighted sequence (A), with central necrosis, an intermediate signal on T1-weighted in phase (B) that is lost on T1-weighted out phase (C) (which mean thar contains microscopic fat) and with contrast uptake in the arterial phase (D). A right partial nephrectomy was performed.
Figure 4 – Papillary variant of RCC in a 69-year-old male patient. The MRI shows a low signal on T2-weighted images (A) and CT imaging (axial pre-contrast (B) and corticomedullary (C)) shows a homogeneous, well-defined lesion with low contrast uptake (these tumors tend to present a mean density ranging between 50-60HU in the corticomedullary phase and 65-75HU in the nephrographic phase).
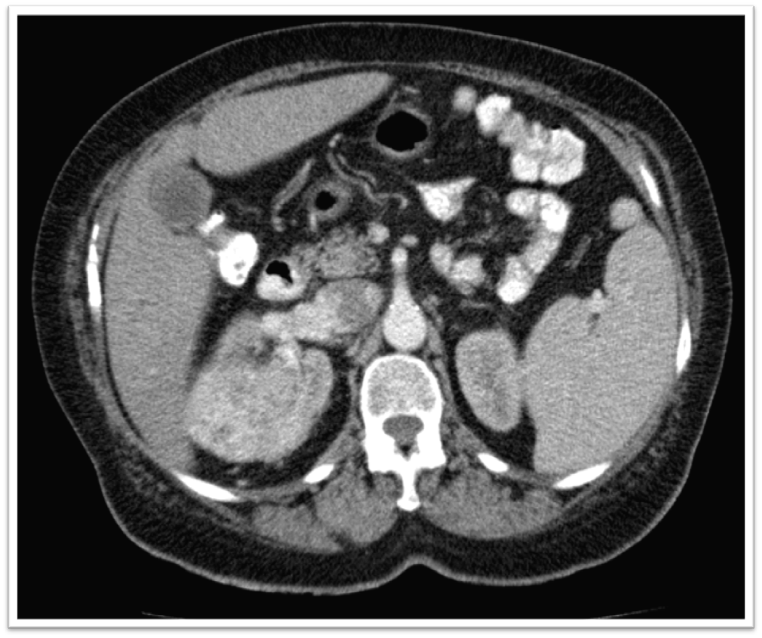
Figure 5 – Chromophobe RCC in a 76-year-old female patient. The CT imaging (axial pre-contrast (A), corticomedullary (B) and nephrographic phases) shows a moderate contrast uptake (80-100HU in the corticomedullary phase, which is less intense than the clear cell variant and more intense with de papillary variant). A central scar may be present (a feature also found in oncocytomas).
Figure 6 – A left partial nephrectomy was performed due to suspected of RCC in a 39-year-old male patient. The anatomopathological result was oncocytoma. The previous MRI (T2-weighted axial (A) and coronal (B) images) (arrow) shows a high / intermediate signal compared to renal cortex and a hypointense central stellate scar. These findings are indistinguishable from those of chromophobe RCC.
Figure 7 – An incidental left renal lesion, in a 71-year-old male patient, was found in MRI performed to evaluate the prostate (A) (arrow). After, the tumor was characterized by CT imaging (axial pre-contrast (B) and corticomedullary phase (C)) that shows a clear cell RCC. A tumor enucleation was performed and one year later a local recurrence was detected (D, E).
Figure 8 – Clear cell RCC in a 65-year-old male patient with von Hippel-Lindau disease with intrathyroid clear cell renal carcinoma metastasis and papillary thryroid carcinoma (not shown). The CT imaging (axial pre-contrast (A), corticomedullary (B) and nephrographic (C) phases) shows an expansile heterogeneous lesion in right kidney with cystic areas and solid component with intense contrast uptake at the corticomedullary phase. A right nephrectomy was performed. Later, a single metastasis appeared in soft tissue on FDG PET/CT (D, E) (arrow).
Figure 9 – Status post right nephrectomy for clear cell RCC in a 68-year-old male patient. Three years later, pulmonary (not shown) and right adrenal metastases clear cell RCC were detected. A right adrenalectomy was performed.
Figure 10 – Clear cell RCC in a 73-year-old female patient. CT imaging (axial corticomedullary phase) shows a clear cell RCC in the right kidney thar extents into the inferior vena cava.
The RCC subtypes have different imaging features that should be recognized by radiologists because of implications for clinical management. In some cases, a confident radiological diagnosis may even avoid the use of invasive procedures. The recognition of early stages of RCC allows less aggressive approaches. References 1. Abou Elkassem, A. M., Lo, S. S., Gunn, A. J., Shuch, B. M., Dewitt-Foy, M. E., Abouassaly, R., Vaidya, S. S., Clark, J. I., Louie, A. V., Siva, S., Grosu, A.-L., & Smith, A. D. (2021). Role of imaging in renal cell carcinoma: A multidisciplinary perspective. Radiographics: A Review Publication of the Radiological Society of North America, Inc, 41(5), 1387–1407. https://doi.org/10.1148/rg.2021200202 2. B. Ljungberg (Chair), L. Albiges, J. Bedke, A. Bex (Vice-chair), U. Capitanio, R. H. Giles (Patient Advocate), M. Hora, T. Klatte L. Marconi, T. Powles, A. Volpe Guidelines Associates: Y. Abu-Ghanem, R. Campi, S. Dabestani, S. Fernández-Pello Montes, F. Hofmann, T. Kuusk, R. Tahbaz Guidelines Office: N. Schouten, E-J. Smith. (2023). EAU guidelines on renal cell carcinoma. https://uroweb.org/guidelines/renal-cell-carcinoma 3. Low, G., Huang, G., Fu, W., Moloo, Z., & Girgis, S. (2016). Review of renal cell carcinoma and its common subtypes in radiology. World Journal of Radiology, 8(5), 484. https://doi.org/10.4329/wjr.v8.i5.484 4. Lyske, J., Mathew, R. P., Hutchinson, C., Patel, V., & Low, G. (2021). Multimodality imaging review of focal renal lesions. The Egyptian Journal of Radiology and Nuclear Medicine, 52(1). https://doi.org/10.1186/s43055-020-00391-z 5. Morshid, A., Duran, E. S., Choi, W. J., & Duran, C. (2021). A concise review of the multimodality imaging features of renal cell carcinoma. Cureus, 13(2). https://doi.org/10.7759/cureus.13231 6. Muglia, V. F., & Prando, A. (2015). Renal cell carcinoma: histological classification and correlation with imaging findings. Radiologia Brasileira, 48(3), 166–174. https://doi.org/10.1590/0100-3984.2013.1927 7. van Oostenbrugge, T. J., Fütterer, J. J., & Mulders, P. F. A. (2018). Diagnostic imaging for solid renal tumors: A pictorial review. Kidney Cancer, 2(2), 79–93. https://doi.org/10.3233/kca-180028 8. Vig, S. V. L., Zan, E., & Kang, S. K. (2020). Imaging for metastatic renal cell carcinoma. The Urologic Clinics of North America, 47(3), 281–291. https://doi.org/10.1016/j.ucl.2020.04.005