Renal Ablation – Update of Current Guidelines and Impact on the Interventionalist
Renal Ablation – Update of Current Guidelines and Impact on the Interventionalist
Raymond Chung, Sivasubramanian Srinivasan
The European Association of Urology recently updated the guidelines (2023) on renal cancer treatment. Recommendations include those pertaining to radiological imaging, tissue diagnosis and the role of thermal ablation in their management. This poster aims to highlight those that may impact the Interventional Radiologists’ pathway in managing these patients. In addition, we aim to provide an educational primer on multiple practical facets of renal tumour management including imaging, choice of thermal ablation techniques in renal cell tumours and simple concepts in mitigating complications.
In this poster, current Society recommendations on the treatment of renal cell carcinoma (RCC) specifically those impacting the Interventional Radiologist will be discussed. - Imaging evaluation o Pre-procedure imaging: In addition to diagnosing, characterising and staging disease; these provide the basis for anatomical classification systems such as Preoperative Aspects and Dimensions Used for an Anatomical (PADUA) classification system and the R.E.N.A.L. nephrometry score. Looking at tumour size, location, relation to the collecting system and exophytic/endophytic nature, the systems can provide objective prognostication of possible morbidity following percutaneous ablation/nephron sparing surgical procedures. Whilst there is no recommended maximum time frame from last imaging to invasive treatment, growth rate of SRMs may be considered. Clear-cell RCC typically grow faster (0.25cm/year), although up to 82% of malignant SRMs can undergo rapid growth (volume doubling) [366]. o Post treatment surveillance: Individual risk based assessment will determine the level of scrutiny required in the post-procedure imaging. For localised RCC, considering a potential higher local recurrence rate after percutaneous thermal ablation therapy, a more rigorous imaging follow-up regime is suggested. Whilst there is no evidence-based standard, a suggested regime for high-risk local recurrence is CT evaluation at 3 and 6 months, followed by 6 monthly to 2 years, yearly to 5 years and biennial beyond 5 years. Conversely, expert consensus from Asia suggests 6 monthly imaging to 2 years with subsequent yearly imaging evaluation up to 5 years. - Role and timing of renal biopsy. o Percutaneous tumour biopsies are beneficial for: Histological diagnosis of indeterminate radiological renal lesions. Identifying patients suitable for active surveillance by evidence of tumour grade and histotype. Histology prior to time of percutaneous ablation therapy is preferred as this reduces the rates of unnecessary treatment. In a series of 182 patients, 27.5% of patients avoided further invasive treatment (surgery or ablation) due to a benign diagnosis from the biopsy specimen. Identifying the treatment algorithm in metastatic disease. o Recommended biopsy techniques include: Using a coaxial technique for core biopsy – 18 gauge needles are sufficient for tissue diagnosis. Ideally, a minimum of two good quality cores should be acquired from the solid enhancing components avoiding central necrotic areas. Fine needle aspiration is not recommended. Performing biopsy of cystic renal tumour masses only if there is an appreciable soft tissue target. - Choice of Thermal Ablation: o Size, location and vascularity are the main denominators in deciding the thermal ablation technique. o Typically, lesions under 3cm can be managed with similar local recurrence risk by RFA, MWA or cryotherapy. o Larger lesions are better treated via MWA or cryotherapy given the ability to create larger ablation zones. Pre-ablation embolisation may be considered in those with hypervascularity rendering risk of either heat sink effect and subsequent reduced ablation or bleeding post ablation, the latter more associated with cryotherapy. o For centrally located tumours, cryoblation is preferred given the reduced risk of urothelial injury. - Common thermal ablation complications and how to avoid them. o Avoiding thermal injury to the collecting system is especially important in relation to the pelvi-ureteric junction and adjacent proximal ureter. Options include retrograde pyeloperfusion [Fig. 1] and choosing cryotherapy as the ablative therapy mode. o Thermal injury to adjacent organs, typically bowel, may be manipulated by a combination of patient positioning, hydro-/pneumodissection [Fig. 2] and, balloon interposition insufflation.
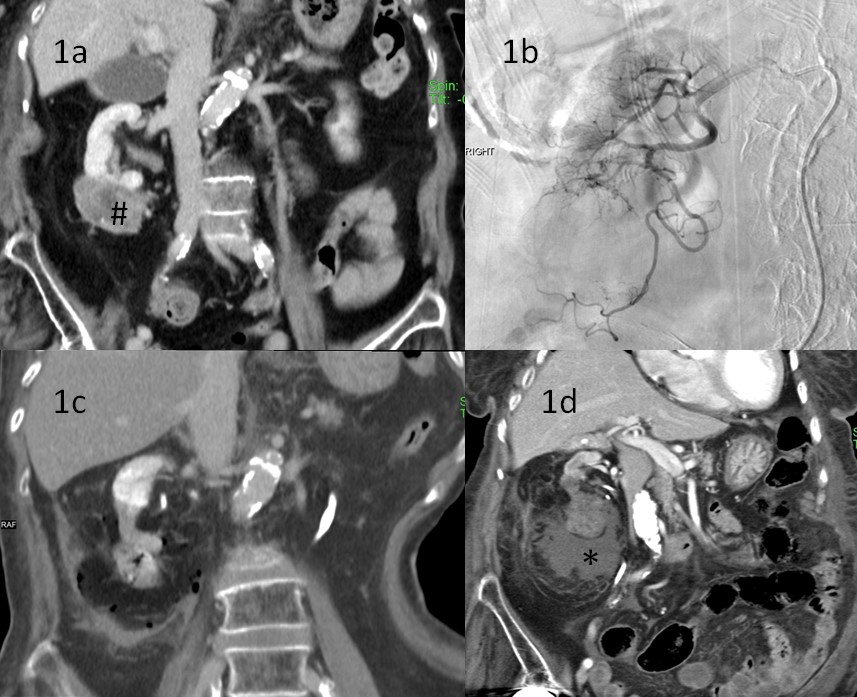
Fig. 1: Percutaneous treatment of a 5.4cm lower pole renal cell carcinoma. (a) Coronal CT of an exophytic right lower pole RCC (#). (b) Digital subtraction angiography - step 1: pre-ablation embolization given size and vascularity. (b) Coronal CT - step 2: post overlapping percutaneous MWA of the tumour – wide ablation margin encapsulating part of the collecting system. (c) Follow up coronal CT: complete ablation of the right RCC but with thermal injury to the pelvicalyceal system resulting in persistent urinary leak. This was treated by retrograde ureteric stent insertion and percutaneous drainage of the urinoma (*). Learning point: retrograde pyeloperfusion of the pelvicalyceal system and more judicial ablation would have helped mitigate the subsequent pelvicalyceal injury.
Fig. 2: Percutaneous treatment of a 2.9cm left renal tumour. (a) Axial CT of an enhancing left renal tumour, histologically confirmed RCC. (b) Pre-ablation CT delineating the adjacent colon next to the left RCC. (c) Patient positioned right lateral decubitus, 18G needle inserted between the RCC and colon for pneumodissection with carbon dioxide. (d) Additional dilute contrast (*) injection for additional hydrodissection. (e) Percutaneous needle ablation through the RCC with satisfactory protective margin from the colon. Learning point: if there is less than 0.5cm between bowel loop and RCC margin, protective measures are recommended.
Surgical management remains the mainstay of treatment in the majority of renal tumour cases whilst percutaneous techniques are typically reserved for those with greater co-morbidities and higher risk of renal function loss post surgery. The Interventionalist is therefore often left facing ablation of renal tumours with an overall more complex patient profile. Understanding the current guidelines, the impact of these on the patient treatment pathway and optimising percutaneous techniques to maintain good outcomes, avoiding complications and unnecessary procedures is imperative in these higher risk groups.