MRI comparison of the two most actual classifications of the Mullerian anomalies
MRI comparison of the two most actual classifications of the Mullerian anomalies
Dr. Dayana Yankova-Pushkarova and Prof. George Hadjidekov
The aim of this poster is to compare the advantages and disadvantages of the two most actual classification systems on practical basis with clinical illustrations on 3T magnetic resonance imaging. To make a brief review of the principles of categorization of both systems. To show the pros and cons of both classifications according to literature sources and on our own opinion based on practice.
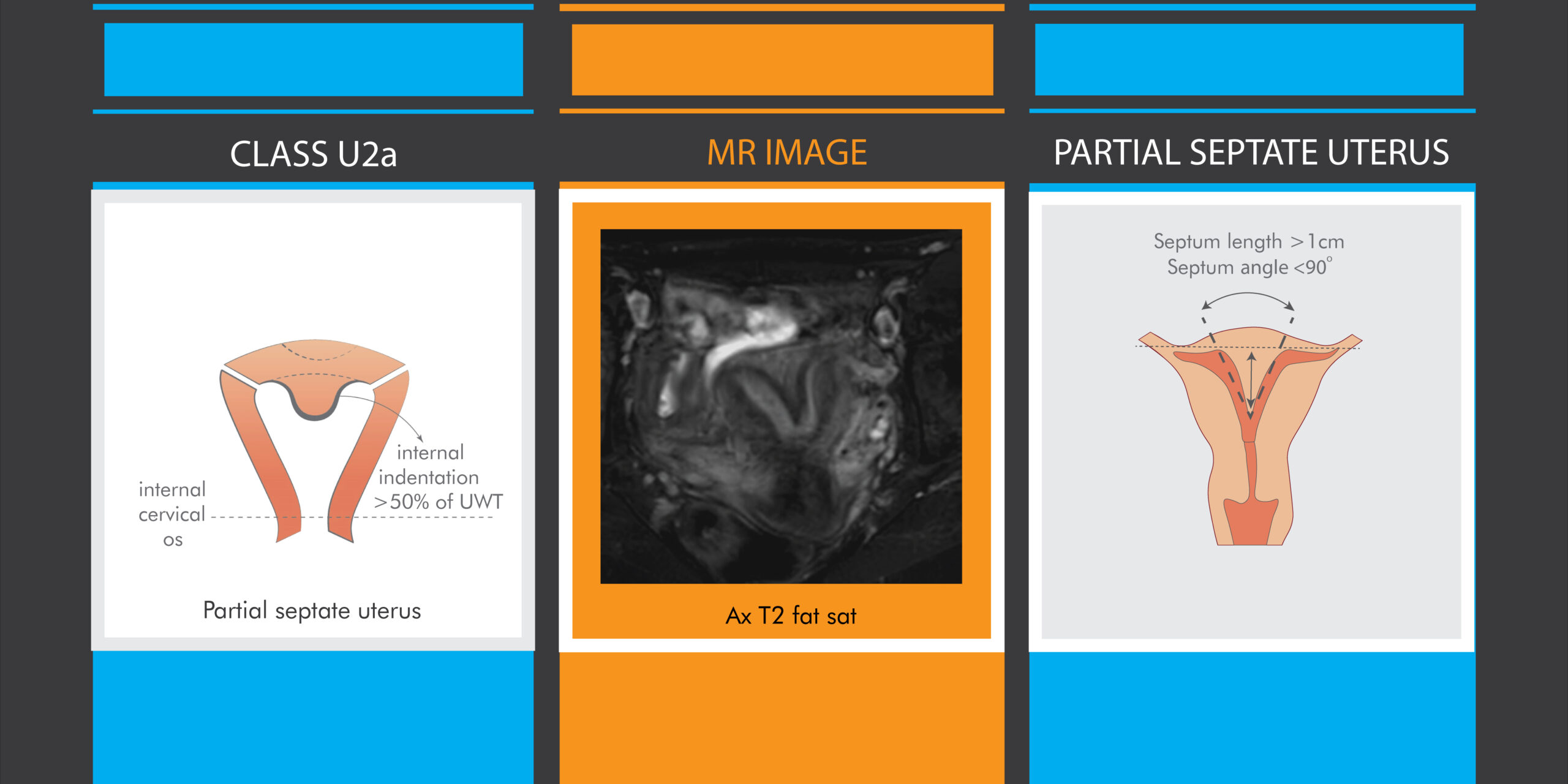
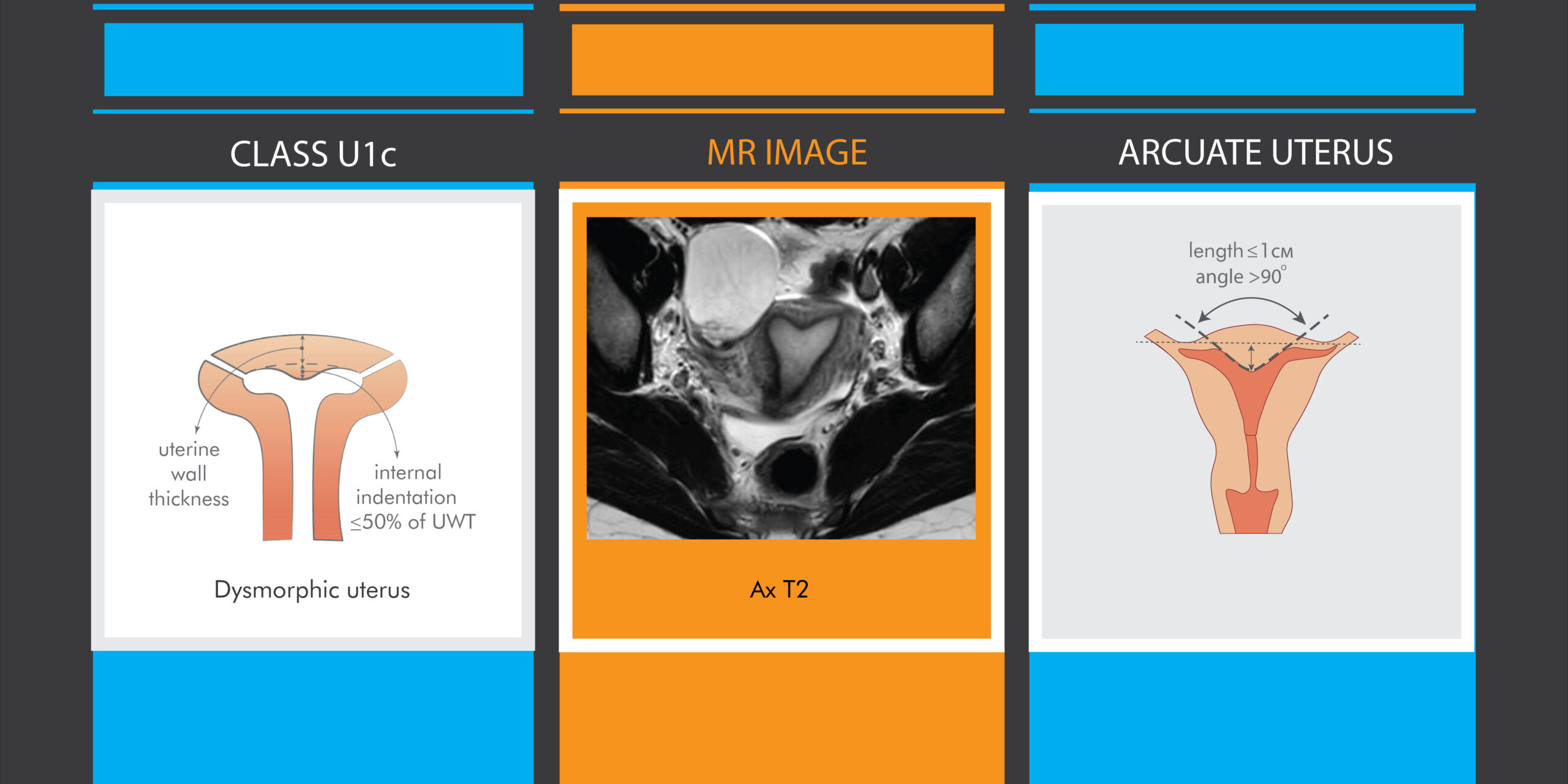
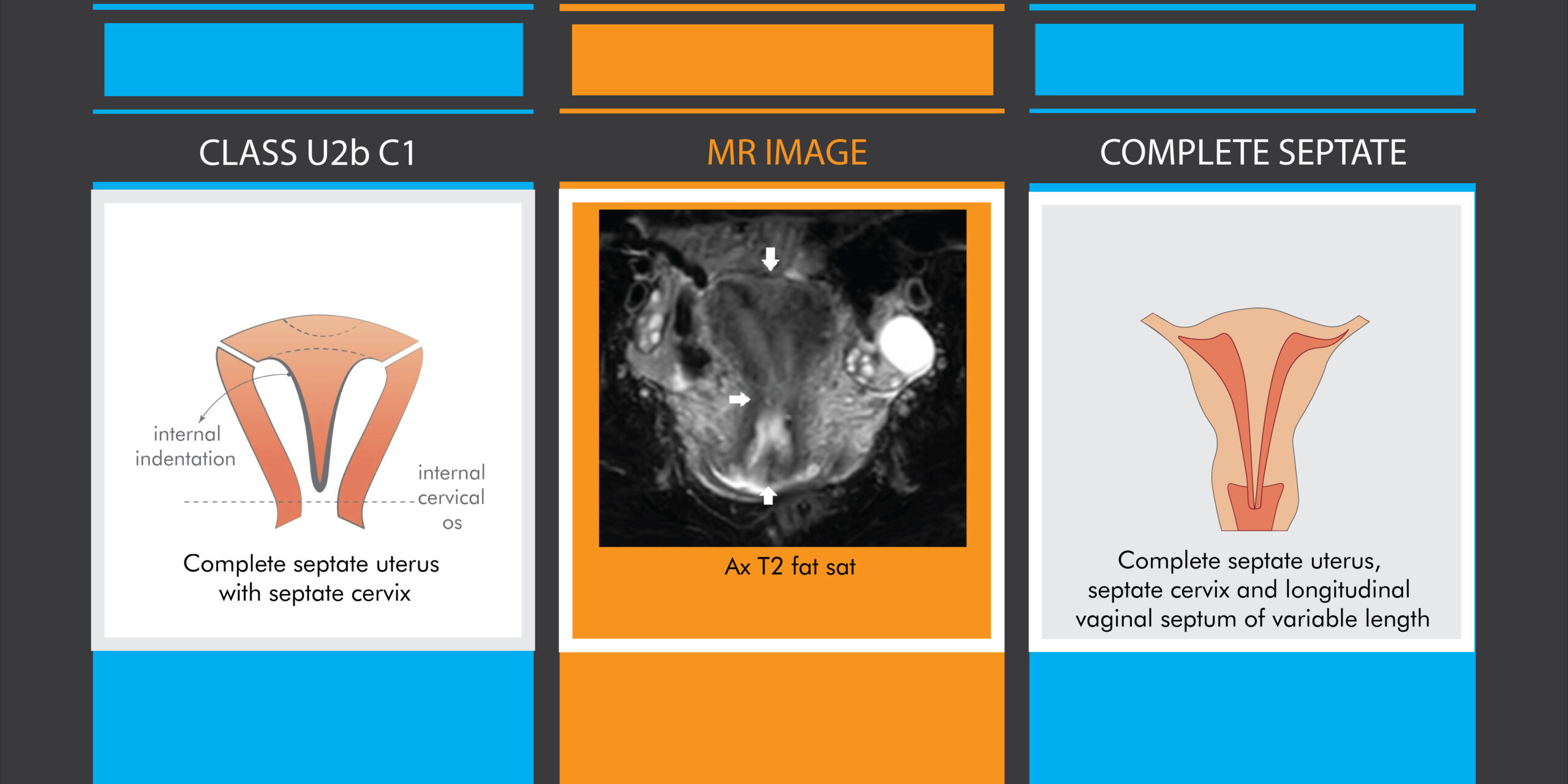
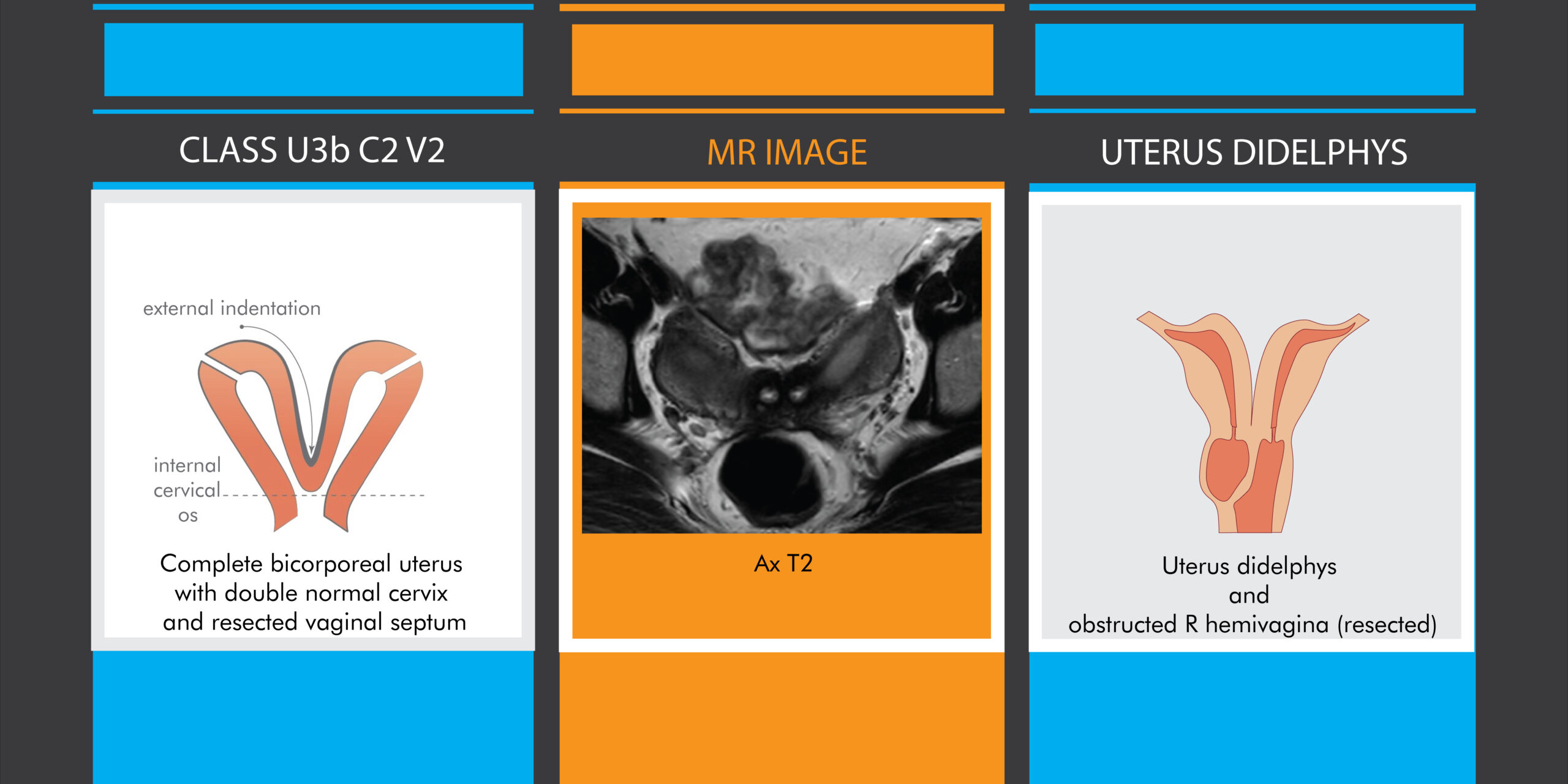
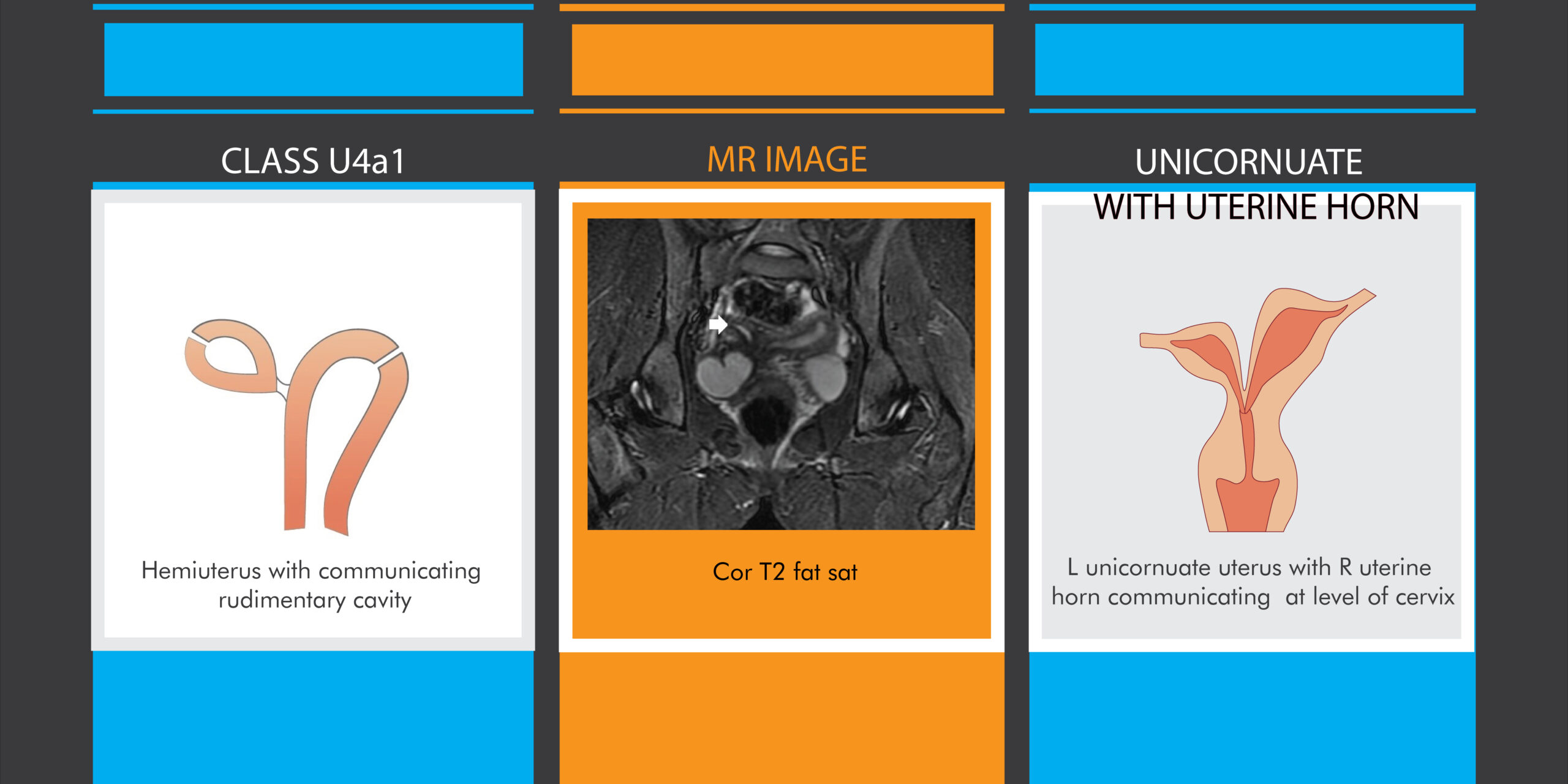
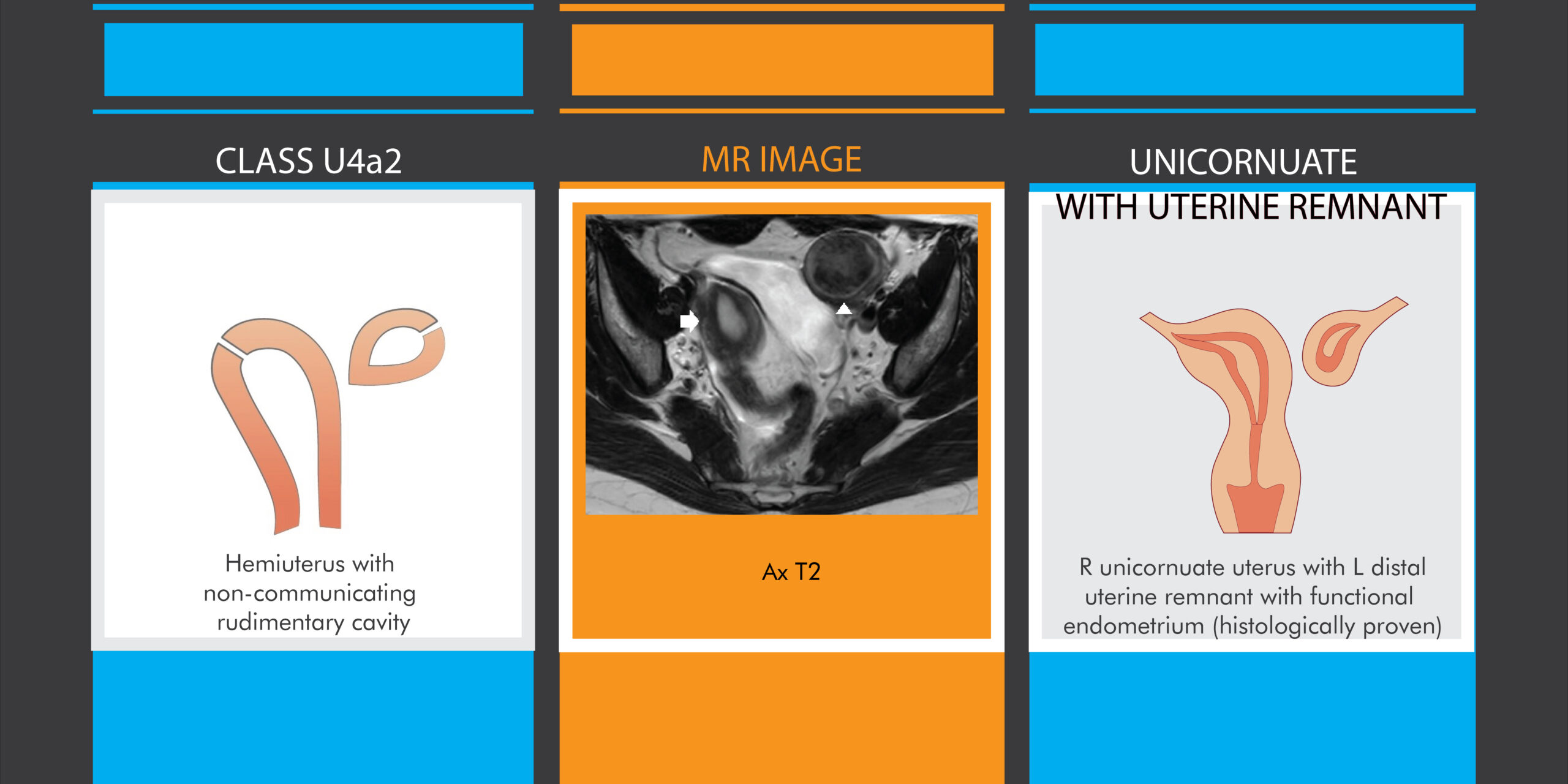
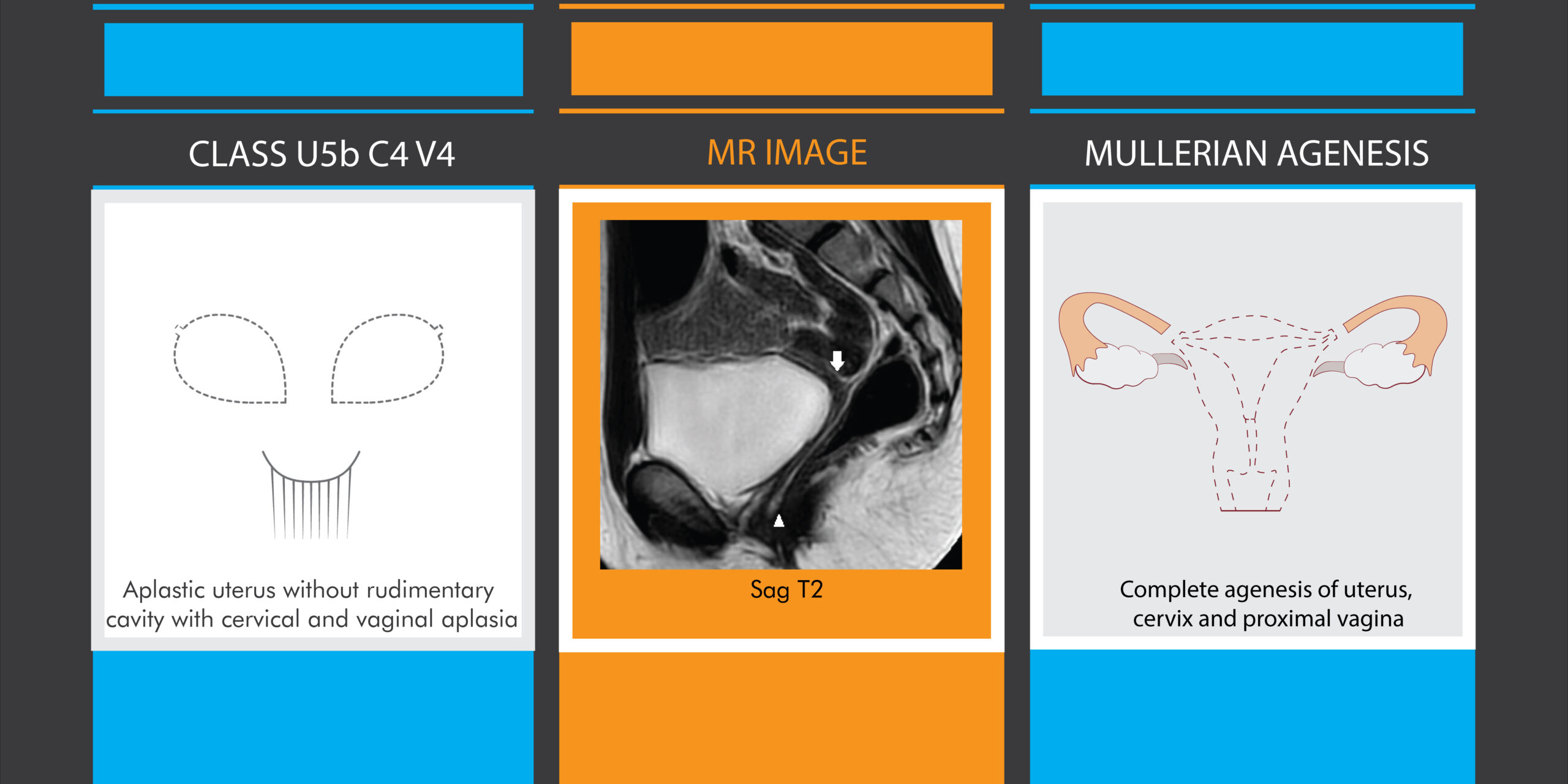
Congenital anomalies of the female genital tract with mullerian origin are relatively common in practice as a pathologic group, despite of their wide intragroup range of frequency, clinical presentation, imaging appearance and female health consequences – from cyclic pelvic pain to primary infertility. The variety of the Mullerian duct anomalies requires creation of up to date, comprehensive and practical classification of this complicated pathology. The latest recognized attempts encompass the European Society of Human Reproduction and Embryology (ESHRE) and the European Society for Gynecological Endoscopy (ESGE) consensus of female genital tract congenital anomalies /2013/ and the American Society of Reproductive Medicine (ASRM) Mullerian anomalies classification / MAC 2021/. The ESHRE/ESGE classification system from 2013 is simple, easy to use anatomy-based and embryology-oriented categorization system. It focuses on the characterization of the uterine anomalies in 6 main classes with independent cervical and vaginal subclasses giving the opportunity of extensive variety of combinations between these entities. The system includes concrete criteria for measurement with some exceptions raising the risk of overdiagnosis and unnecessary treatment. The newest ASRM Mullerian anomalies classification (MAC) from 2021 is more clinically related with pregnancy outcome and treatment options. ASRM MAC 2021 is based on the classical American Fertility Society classification /AFS 1988/ improved with new categories including cervical, vaginal and complex anomalies. The educational and interactive tools of the improved version provide wider range of practical information for radiologists, gynecologists and surgeons. Magnetic resonance imaging (MRI) is a verifying modality for female pelvis examination which demonstrates in detail anatomical deviations from embryological origin of the female reproductive organs. It is the method of choice for evaluation of congenital uterine anomalies [1,2]. MRI has superior role in the delineation of the external uterine contour which is the main difference between two of the main classes – septate and bicornuate/didelphys uterus [3]. According to the literature [4,5,6] the main disadvantage of the ESHRE/ESGE classification system is the possibility for overdiagnosis of septate uterus. It is described as uterus with normal outer contour and internal indentation at the midline of the fundus exceeding 50% of the uterine wall thickness with partial septate uterus septum not reaching the internal cervical os [7,8]. According to this wide definition some cases of small uterine septum with no clinical significance can enter in this category, leading to unnecessary treatment with hysteroscopic metroplasty [9,10]. The ASRM definition of partial septate uterus with septum length over 1 centimeter and septum angle under 90 degrees [11] excludes the opportunity of false positive results of septate uterus cases (Fig.1). In our opinion the use of subclass c) of Class U1 dysmorphic uterus according to ESHRE/ESGE should be better defined with appropriate drawings. A better delineation of this subclass could transfer some of the controversial cases of septate uterus to this group of congenital anomalies with a little impact on female reproductive health and no surgical treatment needed. We tried to illustrate this subclass with personal drawing according to the ESHRE/ESGE definition with the idea to include all minor uterine deformities with an inner indentation at the fundal midline not exceeding 50% of the uterine wall thickness [7,8] (Fig.2). We agreed that this subclass corresponds to the definition of arcuate uterus according to the ASRM 2021 with internal indentation under or equal to 1 cm with angle above 90 degrees [11]. The visualized concretization of U1c subclass according to ESHRE/ESGE classification system and its correspondence to the definition of Arcuate uterus of ASRM 2021 classification would potentially decrease the inappropriate categorization of septate uterus and subsequent unnecessary treatment. There is better correlation and agreement for definition of complete septate uterus according to both classification systems. Although we couldn’t find an existing ASRM variant in the expanded category of septate uterus with septate cervix without vaginal septation. In our case a vaginal septa was not proven by the gynecological examination neither seen on MRI (Fig.3). Some authors [3,11] criticize the nomenclature of the classes in the European classification, considering difficult and ineffective to remember letters and numbers instead of conceptual pictures with appropriate description as in the new American classification. In our opinion the ESHRE/ESGE classification system is better arranged on embryological basis giving a wide range of combinations with cervical and vaginal congenital anomalies. On the other hand, this system is quite common and not much concrete, unifying pathologies with completely different appearance in only 1 subclass. For example, according to ESHRE/ESGE the definition of complete bicorporeal uterus corresponds both to uterus didelphys and bicornuate of ASRM 2021 varying with only changes in the subclass of cervical anomaly (C2 or C0) (Fig.4). The possibility to present a drawing with appropriate description of the ASRM classification literally gives you the correct diagnosis, but it has some limitations. The possible combinations of uterine, cervical and vaginal congenital anomalies are immense and even the wide variety of pictures in every ASRM 2021 group couldn’t cover them all. For example in our case of genetically proven Herlin-Werner-Wunderlich (OHVIRA) syndrome there is dominant left cavum communicating with the vagina and rudimentary functional right cavum which ends blindly into a hemo-cavity. We assume that this hemo-cavity is an obstructed right hemivagina, but we don’t find this combination of pathologies in the new ASRM system, so we defined it as a left unicornuate with right uterine horn communicating at the level of the cervix. According to the simplified ESHRE/ESGE classification system this case is Class 4 subclass ”a” communicating uterine horn (Fig.5). Regarding to the other “sub-subclass” of Class 4 subclass “a” – hemiuterus with non-communicating functional rudimentary horn, it clearly correlates with right unicornuate uterus with left distal uterine remnant with functional endometrium (Fig. 6). Fortunately, more of the definite pathologies like Mayer-Rokitansky-Kuster-Hauser syndrome can be easily classified by both classification systems (Fig.7). In summary both classifications has pros and cons. The ESHRE/ESGE classification system is more anatomically oriented which make it easier to use for magnetic resonance diagnosis. The newest ASRM 2021 classification of the congenital Mullerian anomalies looks more clinically oriented in regard to patient management and surgical options. Every classification system can’t cover the wide variety of combinations of congenital anomalies of female genital tract which can be found in the everyday clinical practice. Maybe an universal classification could be a challenging task in respect of this rare and complex pathology.
Fig.1 MRI comparison of partial septate uterus according to both classifications Illustrations: MJ design
Fig.2 MRI comparison of dysmorphic and arcuate uterus according to both classifications Illustrations: MJ design
Fig.3 MRI comparison of complete septate uterus according to both classifications Illustrations: MJ design
Fig.4 MRI comparison of bicorporeal and didelphys uterus according to both classifications Illustrations: MJ design
Fig.5 MRI comparison of hemiuterus and unicornuate uterus with horn according to both classifications Illustrations: MJ design
Fig.6 MRI comparison of hemiuterus and unicornuate uterus with remnant according to both classifications Illustrations: MJ design
Fig.7 MRI comparison of aplastic uterus and uterine agenesis according to both classifications Illustrations: MJ design
Conclusion MRI is the best imaging modality to evaluate congenital Mullerian anomalies according to the actual criteria for categorization with the idea to provide timely diagnosis contributing to appropriate treatment strategies and excellent clinical results [3,12]. The ESHRE/ESGE classification system is more related to MR anatomical categorization while the ASRM MAC 2021 is helpful in decision making of treatment strategy. Knowledge of the strengths and weaknesses of the commonly used classification systems about this specific topic has great practical value for the multidisciplinary team of radiologists, gynecologists, reproductive specialists and surgeons. This paper is granted by the “National program for young and postdoctoral researchers - 2” of the Ministry of Education and Science of Bulgaria and Sofia University “St.Kliment Ohridski”.