Diagnostic dilemmas and mimics of genito-urinary infections on imaging.
Diagnostic dilemmas and mimics of genito-urinary infections on imaging.
Antony Augustine, Auradha chandramohan. Christian Medical College, Vellore, TN, India.
This educational exhibit will aim to: Demonstrate the spectrum of imaging findings of common and uncommon infections of the genito-urinary tract. Demonstrate diagnostic dilemmas and mimics of genito-urinary infections on imaging.
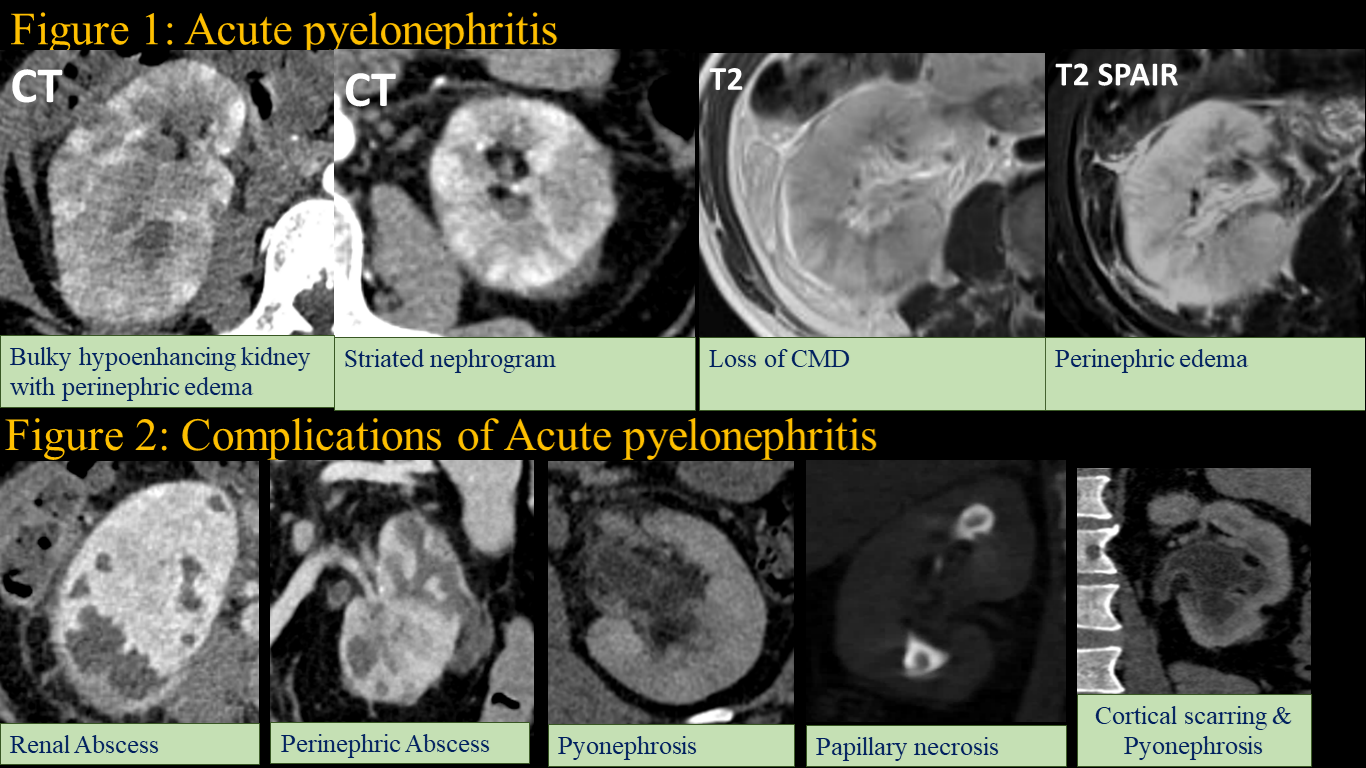
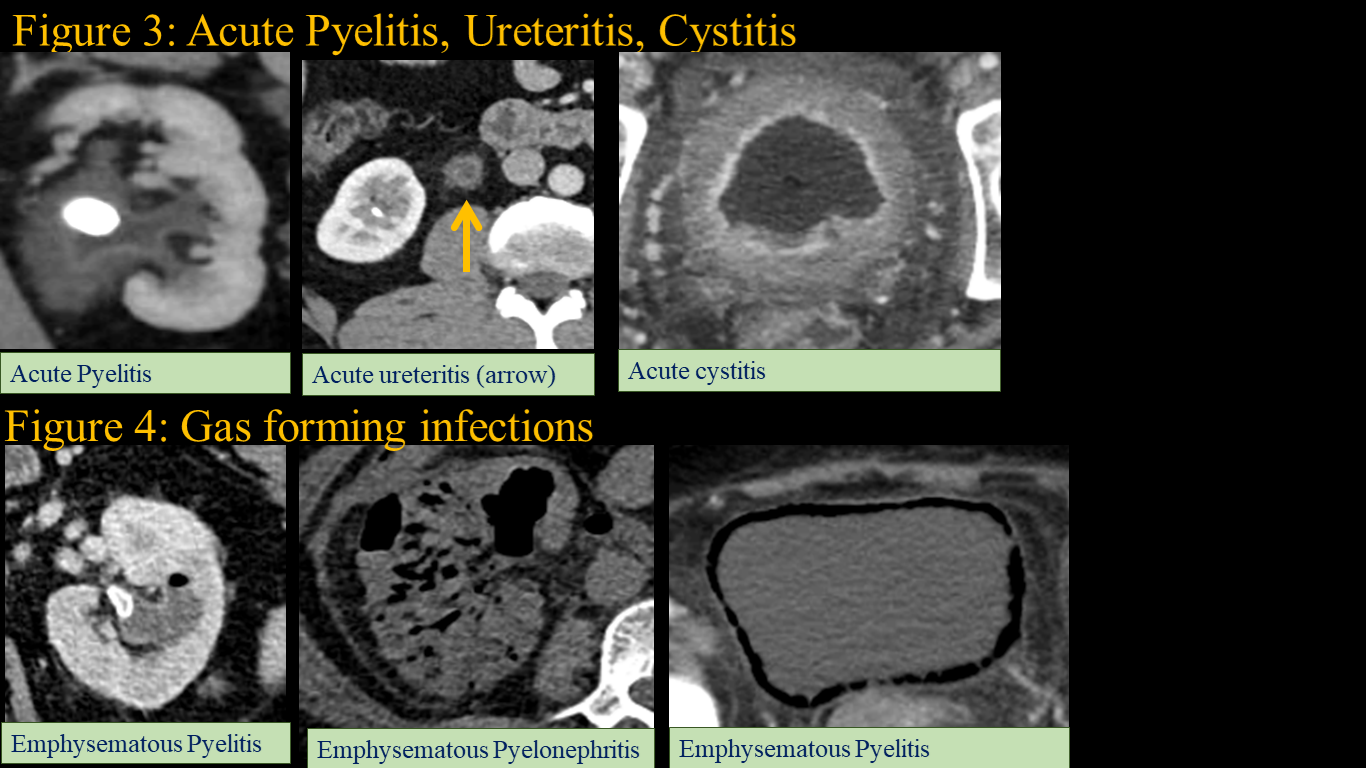
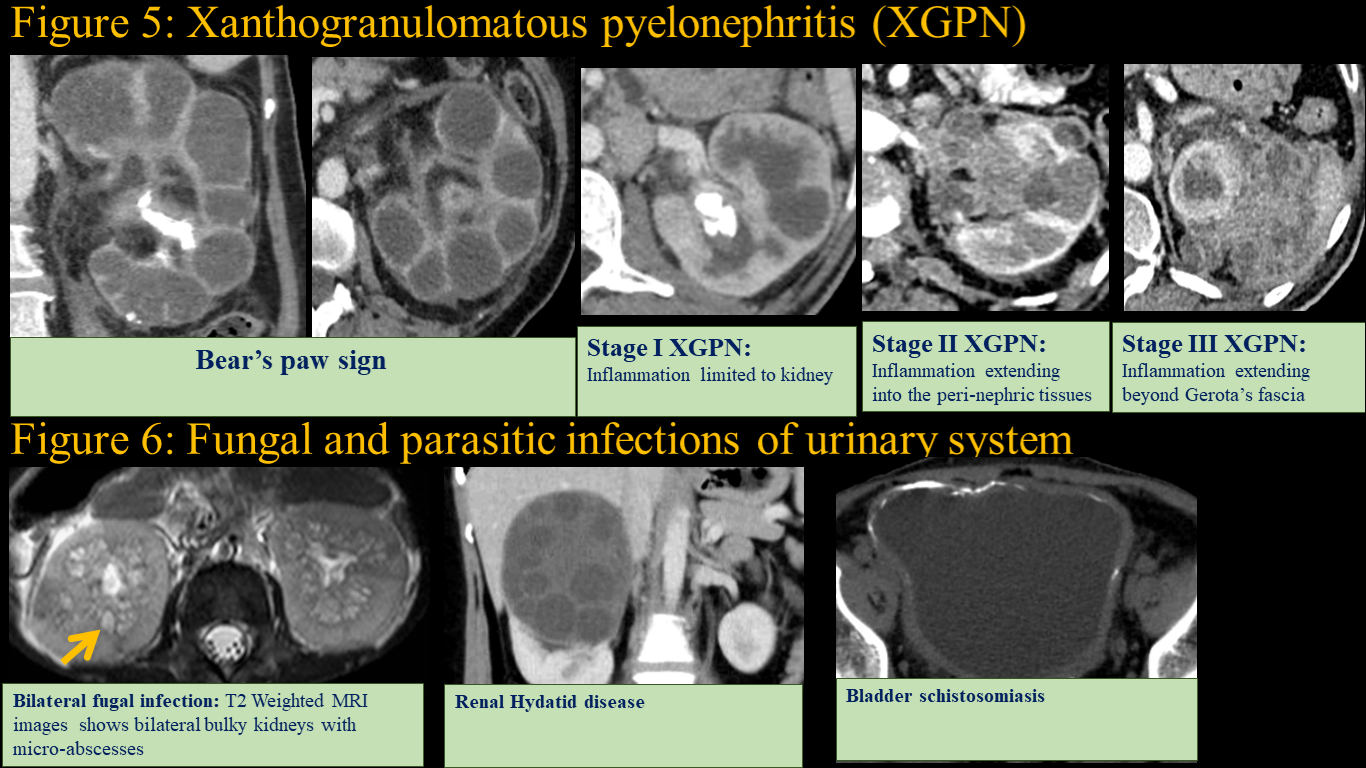
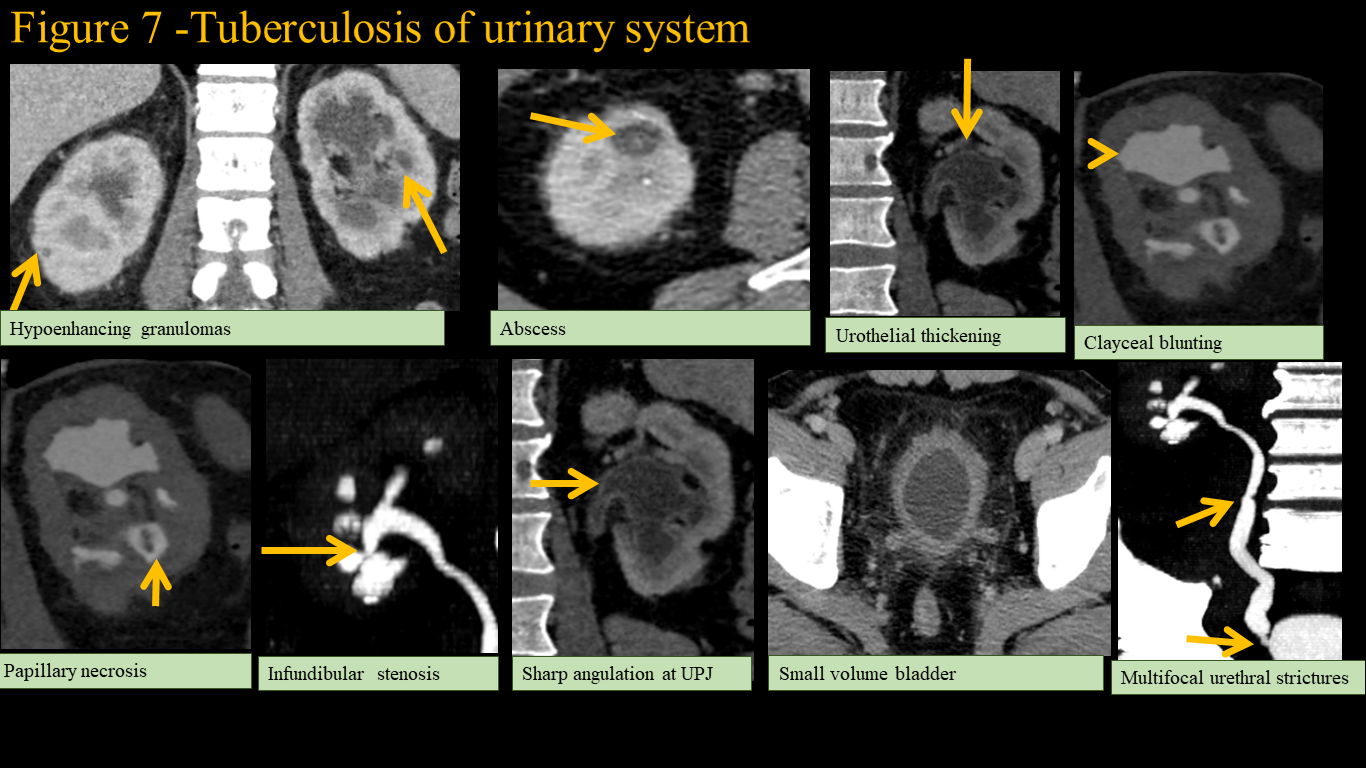
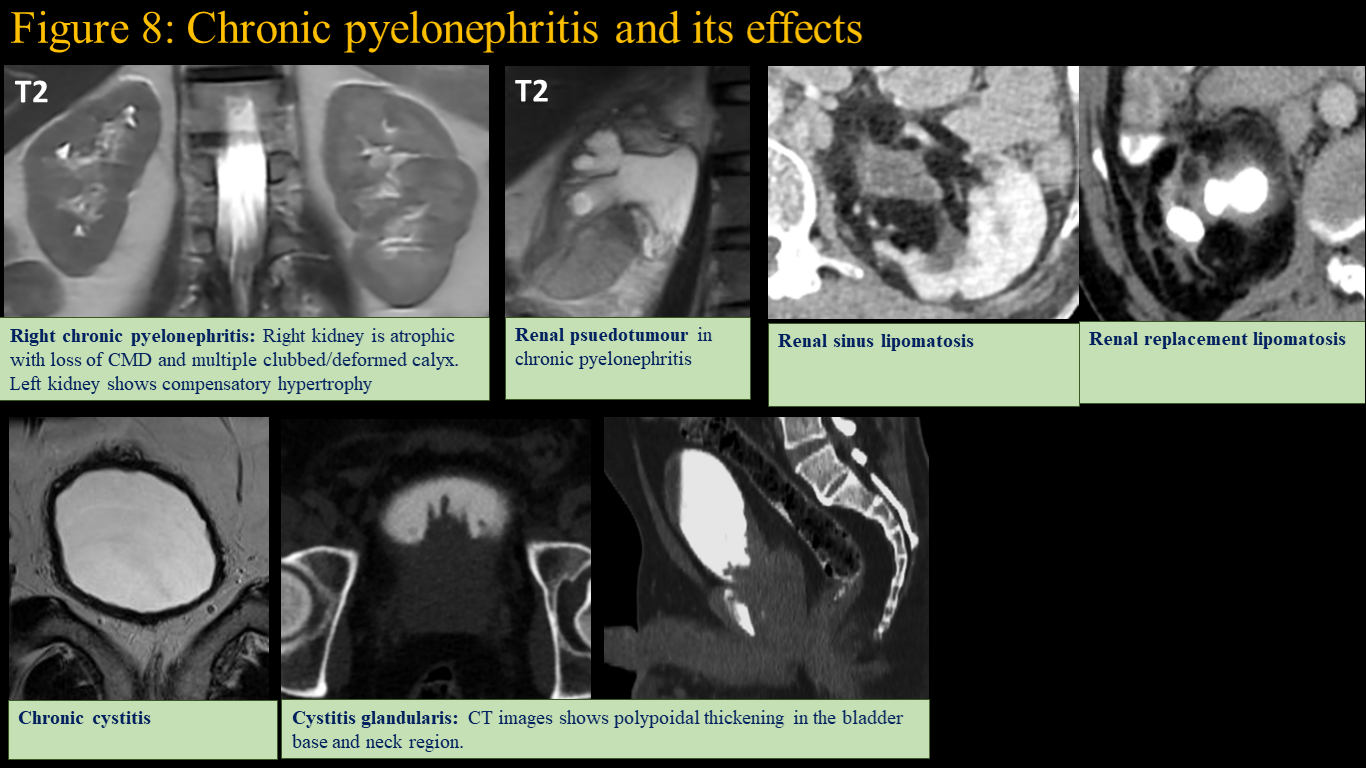
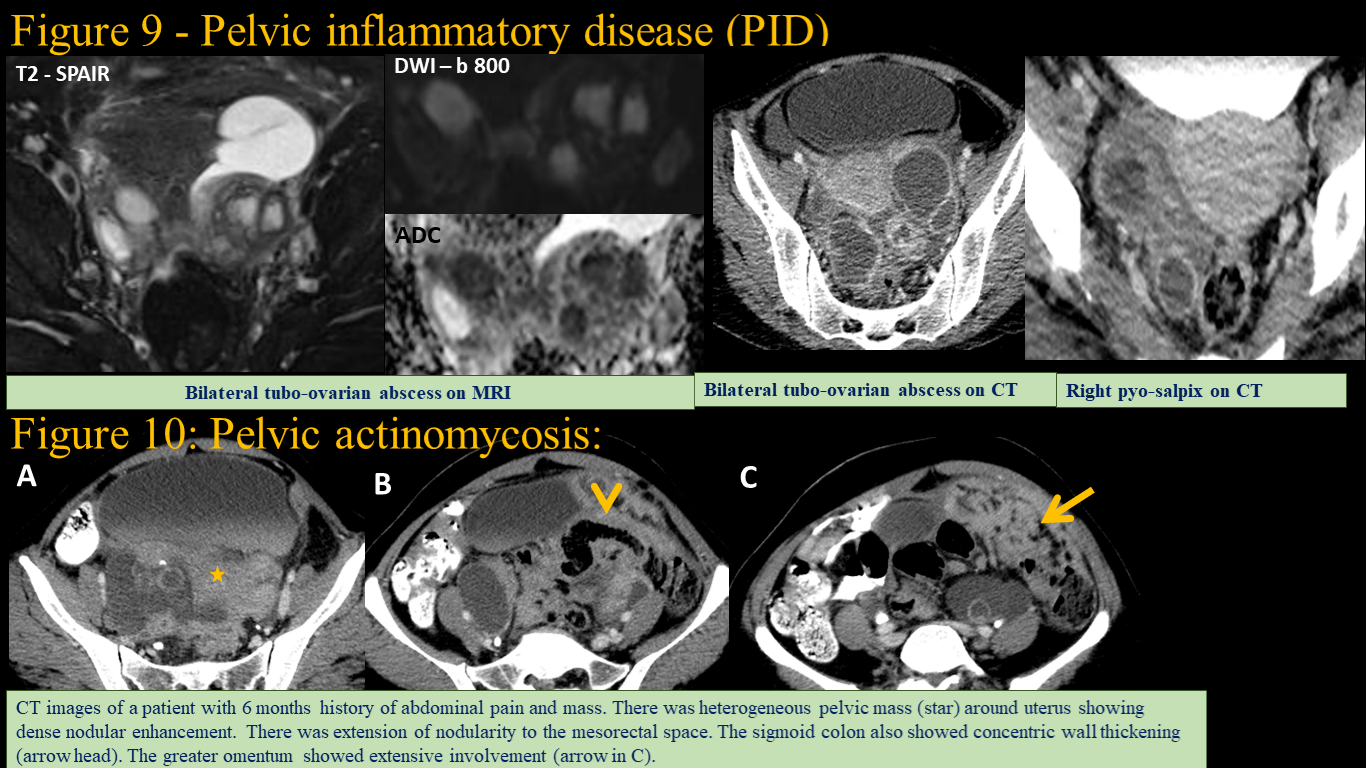
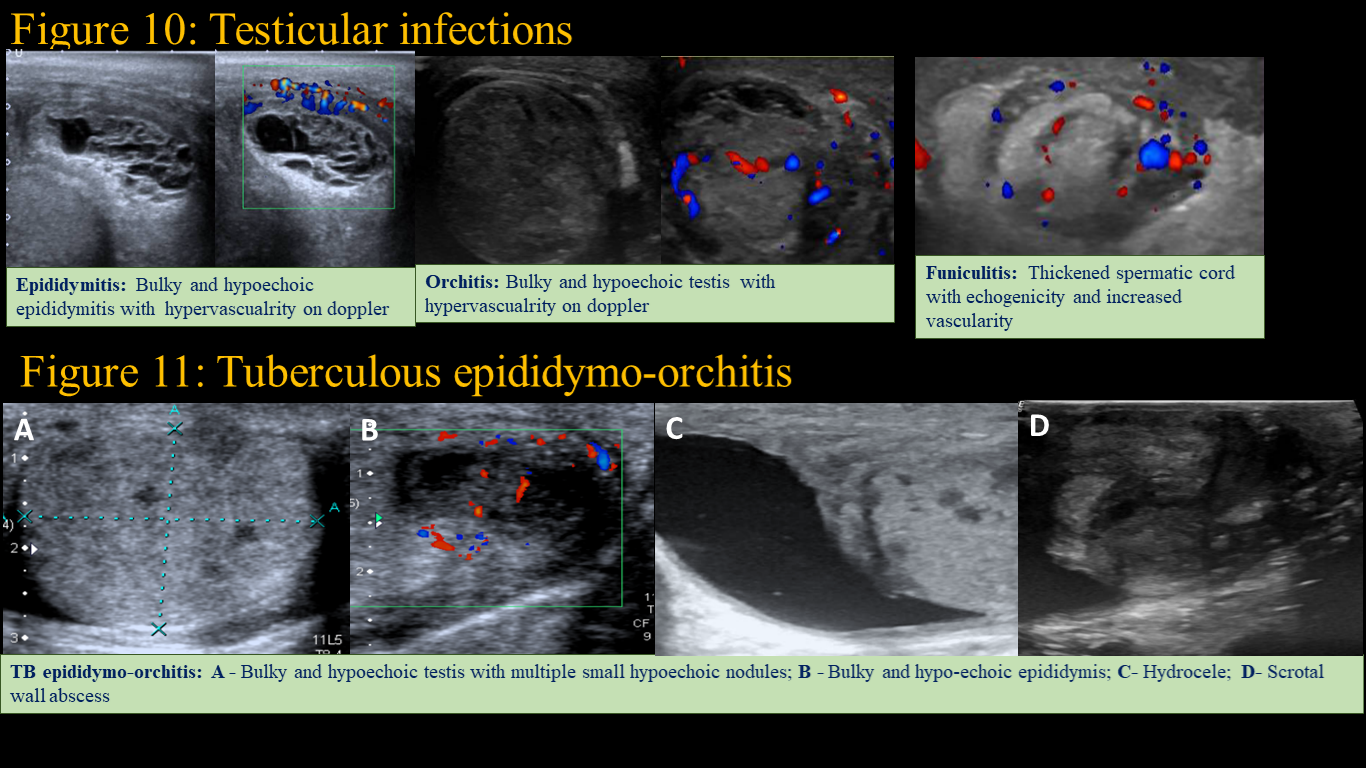
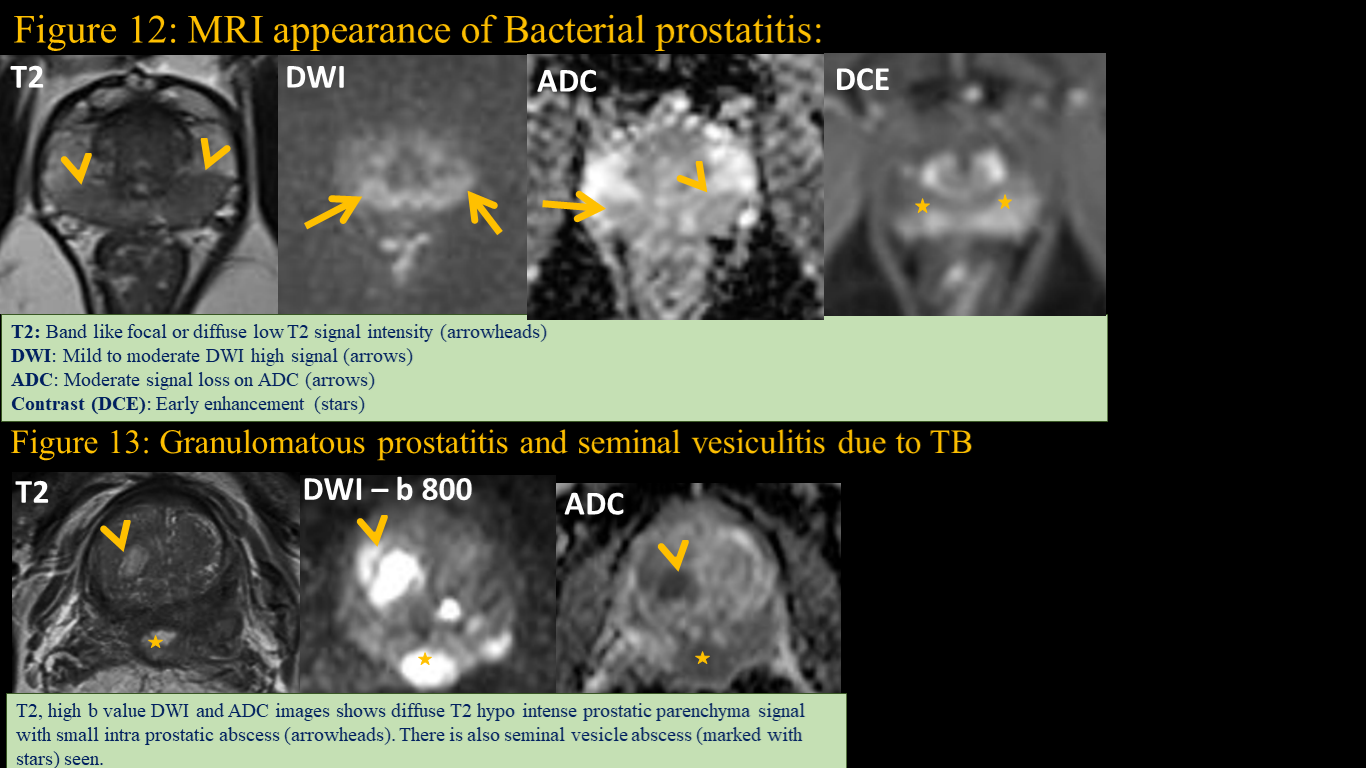
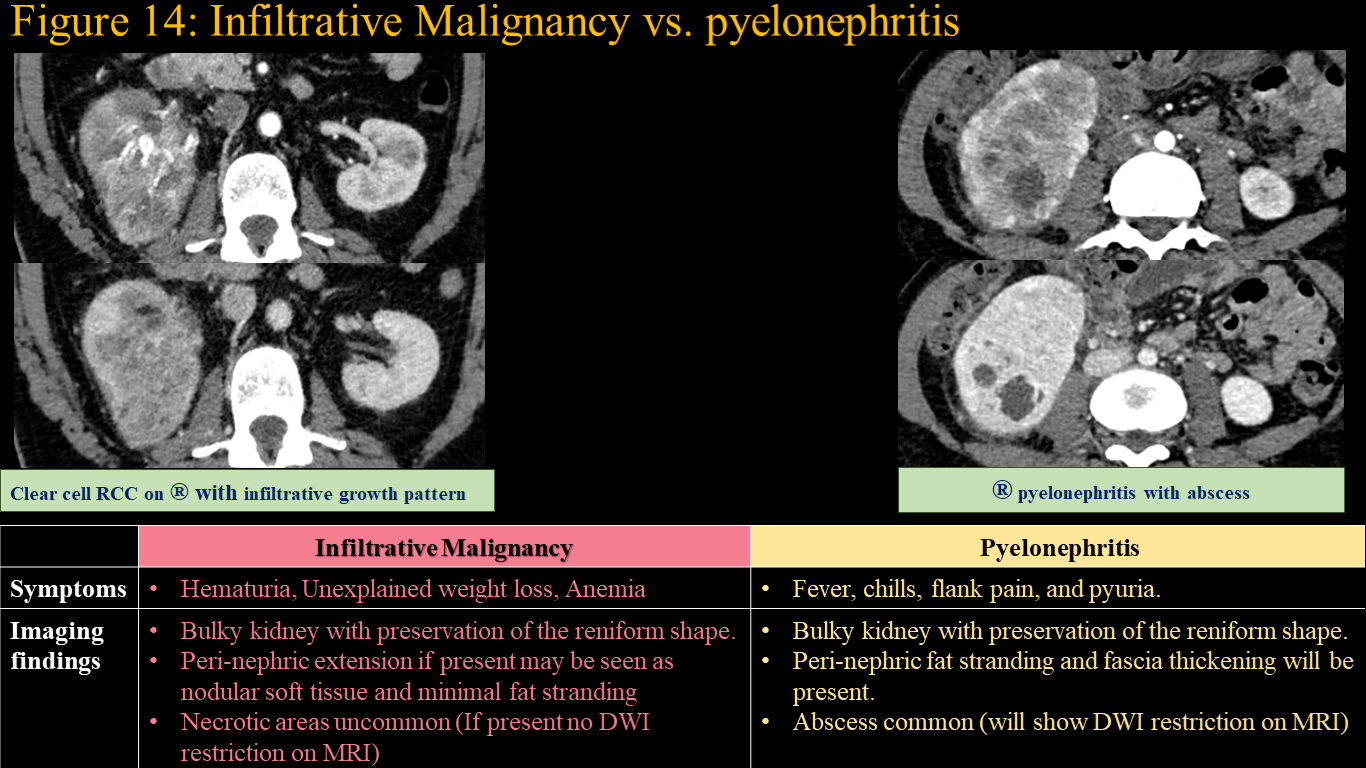
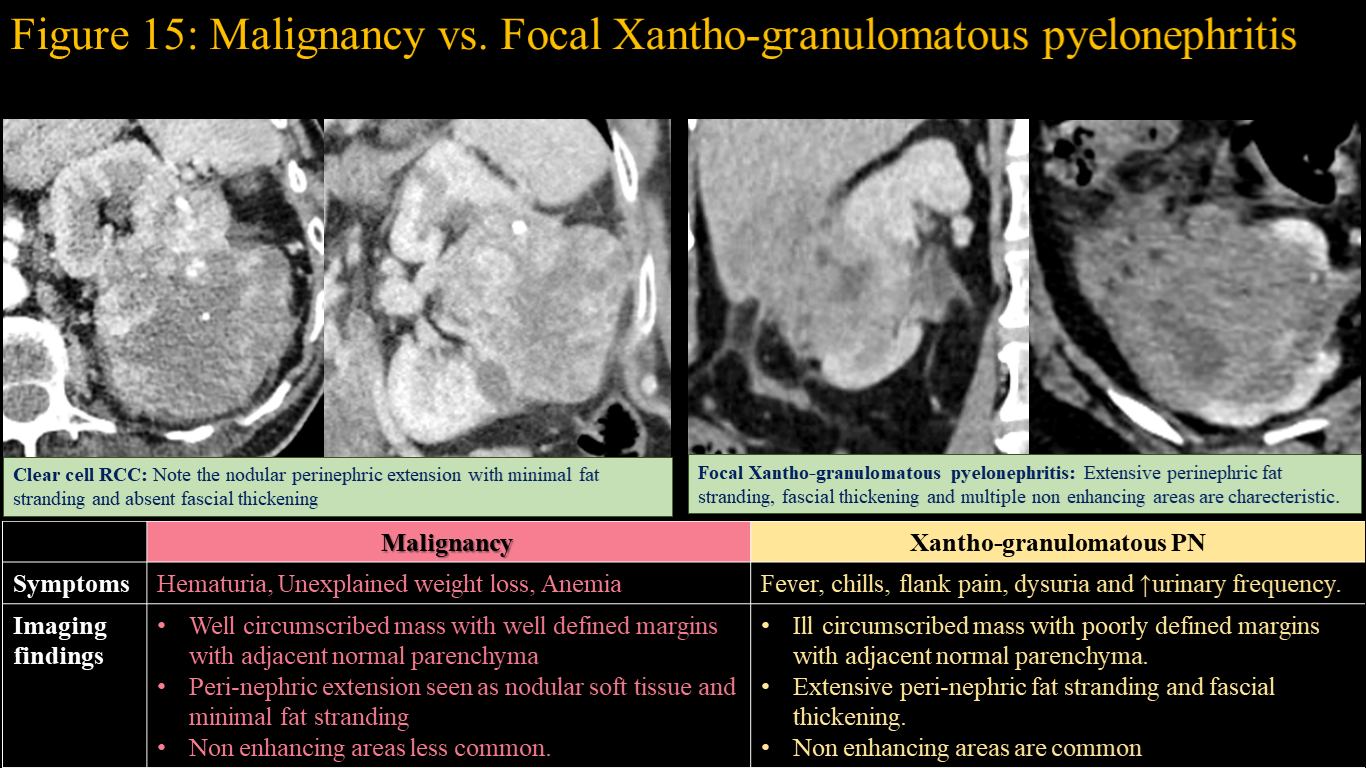
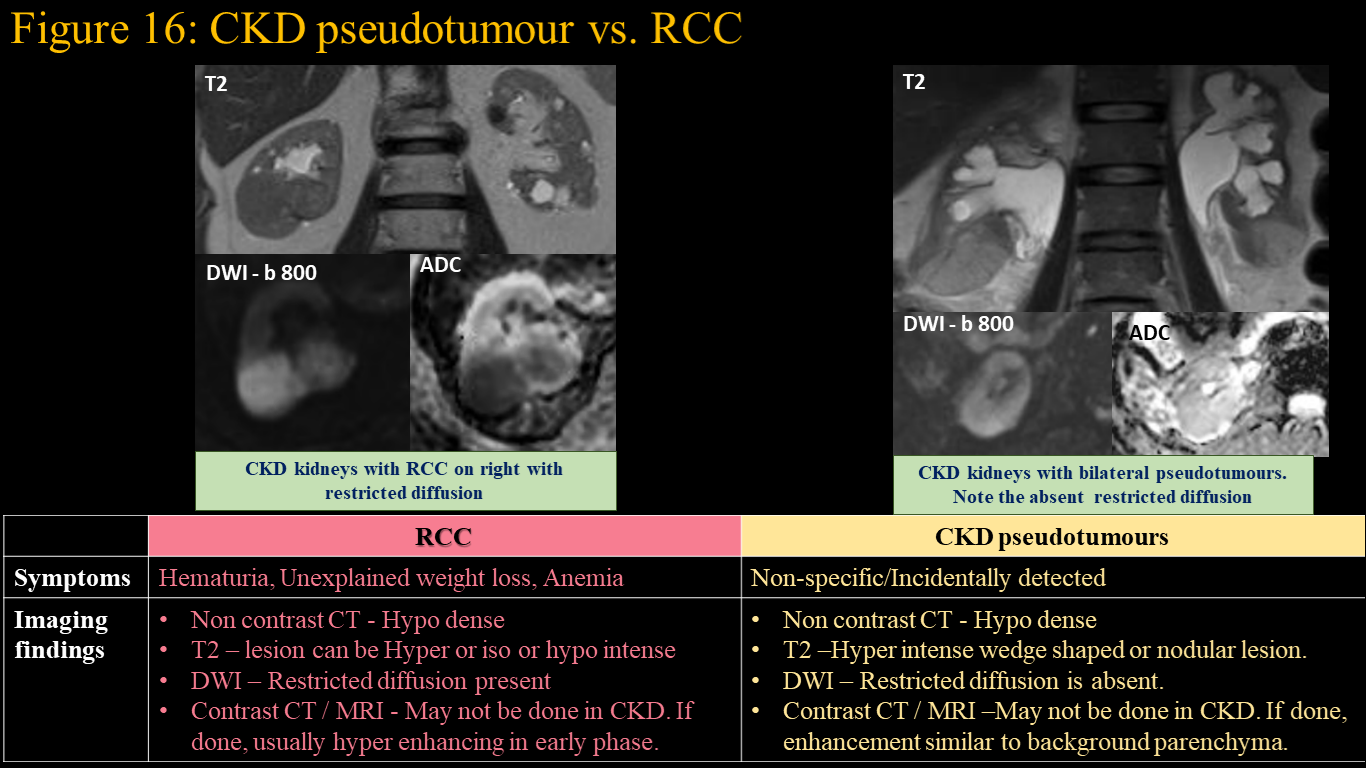
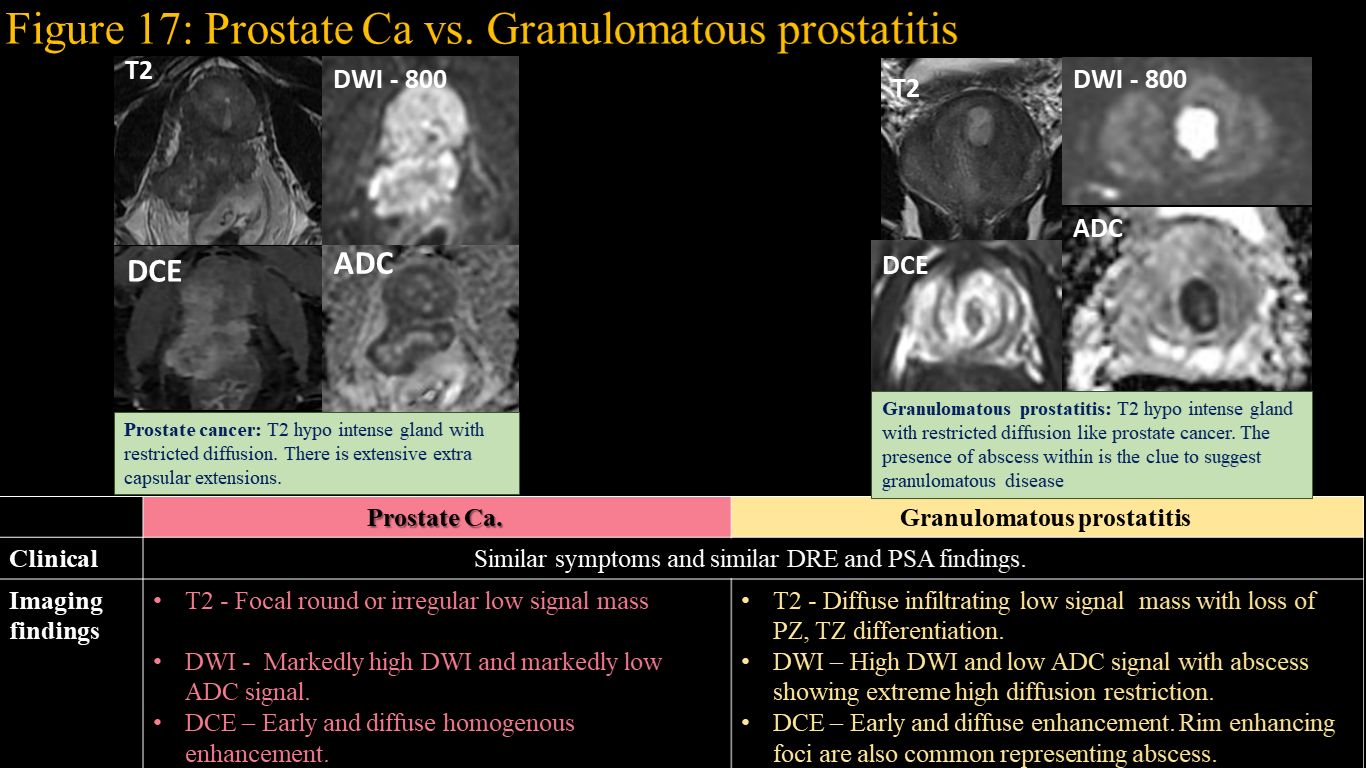
The diagnosis of urinary infections are by clinical and laboratory findings. Imaging is needed; a) if unusual or severe symptoms are noticed, b) in high-risk patients (elderly, diabetics, or immunocompromised), c) No response to intravenous antibiotics within 72 hours and d) repeated infections. The purpose of imaging is to; a) identify conditions that must be cured immediately (Pyonephrosis, Emphysematous pyelonephritis and abscesses), b) to preserve renal function and avoid septic complications, c) Identify cause of UTI (calculus, obstruction, vesico-ureteral reflux, congenital anomalies and cyst infection). Genital infections can be either sexually transmitted or non-sexually transmitted infections. Female genital infections involving uterus, ovaries and tubes are called pelvic inflammatory disease. The diagnosis of genital infections are also by clinical and laboratory findings. Imaging may be needed; a) when uncertain diagnosis on clinical examination, b) Identify Complications Acute pyelonephritis, pyelitis, ureteritis and cystitis: Most cases of acute infections are bacterial caused by Escherichia coli, Proteus mirabilis, and Klebsiella pneumoniae. Typical imaging features of acute pyelonephritis are shown in figure 1. Some of the common complications associated with pyelonephritis is shown in figure 2. Infection of renal pelvis (pyelitis), ureter (ureteritis) and bladder (cystitis) leads to thickening and enhancement at the site with inflammation in adjacent fat as shown in figure 3. Some of the infections can be severe necrotising with formation of gas in tissues. The appearance of such infections are shown in figure 4. Xanthogranulomatous pyelonephritis (XGPN): It is a chronic granulomatous process due to chronic infection inciting a chronic but incomplete immune reaction. Women are more affected than men. Classical imaging findings include a diffusely enlarged kidney with a pelvic or staghorn calculus. The pelvis will be contracted with dilated calyces giving “ bear’s paw sign” as shown in figure 5. The inflammation can be limited to the kidney (stage I) or can extend into the peri-nephric tissues into peri-nephric space (stage II) or beyond into adjacent organs (stage III). The various stages of XGPN is shown in figure 5. Fungal and parasitic infections: Fungal infections of kidney are severe life threatening infection particularly affecting immunocompromised patients. Common organisms are Candida and Aspergillus, Cryptococcus, and mucor. Imaging finding may be non-specific with changes of pyelonephritis. Micro-abscesses are seen in some cases (Figure 6). Fungal hyphae and inflammatory cells can form fungal ball in upper tracts. Mucor has a tendency to invade vessels and cause infarction. Pneumocystis carini infection in HIV patients presents as diffuse punctate calcifications in kidneys. Parasitic infections affecting urinary system include schistosomiasis and hydatid cysts. Schistosomiasis affects urinary tract leading to calcifications (Figure 6). Hydatid cysts in kidney appear as complex cystic lesion with T2 hypo intense three-layered wall and floating membranes / daughter cyst or heterogeneous debris (Figure 6). Tuberculosis of urinary system: Urinary tuberculosis, accounts for 15-20% of extra-pulmonary tuberculosis and can result in varied and striking radiographic appearances. Tuberculosis can involve both the renal parenchyma and the collecting system (calyces, renal pelvis, ureter, bladder and urethra) and results in different radiographic appearances. Since the disease commonly is spread hematogenously, the findings are usually bilateral. The various finding in urinary tuberculosis are demonstrated in Figure 7. Chronic urinary infections and its effects: Chronic inflammation of kidney would result in atrophy of kidney with loss of CMD. There can be cortical scarring, clubbing of calyx, fat proliferation in and around kidneys. There can be pseudotumour formation in kidneys which represent nodular compensatory hypertrophy of relatively preserved renal parenchyma. Chronic cystitis leads to bladder wall thickening and small capacity. Recurrent bladder infections can lead to mass like thickening of bladder wall due to metaplasia of urothelium they can be plaque like (cystitis cystica) or polypoidal (Cystica glandularis). The imaging appearances of chronic urinary infections are shown in figure 8. Pelvic inflammatory disease: Pelvic inflammatory disease (PID) is a broad term that encompasses a spectrum of infection and inflammation of the female genital tract. Common causative organisms are Chlamydia trachomatis and Neisseria gonorrhoeae. Less common organisms are Mycobacterium tuberculosis and Actinomyces spp. Imaging manifestations of PID are demonstrated in figure 9. Tuberculosis is unique in that, it is associated with diffuse peritoneal involvement (nodular peritoneal thickening, loculated ascites) and enlarged nodes with necrosis and calcifications. Actinomycosis infection causes dense enhancement of inflammatory masses with extensive transfascial inflammatory changes, contiguous adjacent organ involvement and absent nodes (figure 10). Male genital infections: Testicular infections are most common male genital infections. Infections are generally from lower urinary tract source through retrograde spread. Ultrasound is the imaging modality in these conditions Common causative organisms are Chlamydia trachomatis, Neisseria gonorrhoeae and E. coli (most common in elderly). The imaging appearance of testicular infections is demonstrated in image 10. Tuberculous epididymo-orchitis have more insidious onset that rest of the bacterial causes. They are commonly hematogenous and hence bilateral . TB orchitis leads to formation of granulomas in testis seen as multiple hypoechoic nodular foci in testis. Scrotal involvement as abscesses and sinus are also common in TB. Imaging finding in TB orchitis is shown in figure 11. Prostatitis is an inflammatory condition of the prostate. It can be bacterial, granulomatous and IgG4 related prostatitis. Bacterial prostatitis is usually due to intra-prostatic reflux of infected urine. E. coli, Klebsiella, Proteus, and Pseudomonas are common organisms. The MR imaging appearance of bacterial prostatitis is shown in figure 12. Granulomatous prostatitis can be idiopathic, iatrogenic (following TURP), and infective (TB, Treponema pallidum, herpes zoster virus, and fungi like Cryptococcus, Candida, Aspergillus spp). They have peculiar imaging appearance on MRI as shown in figure 13. Diagnostic conondrums in imaging infections in uro-genital system: The imaging appearance of some of the infective conditions of uro-genital system may not be straight forward. Some of the conditions which can mimic urogenital infections are demonstrated in the next few figures with pointers to differentiate them given as tabular form. Figure 14: Infiltrative Malignancy vs. pyelonephritis Figure 15: Malignancy vs. Focal Xantho-granulomatous pyelonephritis Figure 16: CKD pseudotumour vs. RCC Figure 17: Prostate Ca vs. Granulomatous prostatitis
Figure 1 and Figure 2
Figure 3 and Figure 4
Figure 5 and Figure 6
Figure 7
Figure 8
Figure 9
Figure 10 and Figure 11
Figure 12 and Figure 13
Figure 14
Figure 15
Figure 16
Figure 17
We have shown a plethora of infective conditions in the urogenital region. Clinical evaluation and lab findings can give diagnosis of most of these infections. Imaging is helpful when; a) The diagnosis cannot be made clinically with certainty b) The cause of chronic / recurrent infections needs to be ascertained c) There is high risk for complication and needs to be identified. We have demonstrated numerous conundrums that one may face while diagnosing urogenital infections and clues to solve them correctly.