Image guided thermal ablation of T1 renal cell cancer: A single centre experience.
Image guided thermal ablation of T1 renal cell cancer: A single centre experience.
J. Ryan (1), O. Lynch (2), B.B. McGuire (2), C.P Cantwell (1). 1. Department of Radiology, St. Vincent’s University Hospital, Dublin, Ireland. 2. Department of Urology, St. Vincent’s University Hospital, Dublin, Ireland.
Percutaneous image-guided tumour ablation (IGTA) with radiofrequency ablation (RFA), microwave ablation (MWA) and cryotherapy are curative local therapies for T1 renal cell carcinoma (RCC). Although IGTA of T1 RCCs has been carried out for over 20 years, the long-term outcome data available on these patients has been limited to studies with small patient populations. The aim of this study was to evaluate the oncological outcomes and survival times after ablation of T1 RCC in our unit over a 9-year period.
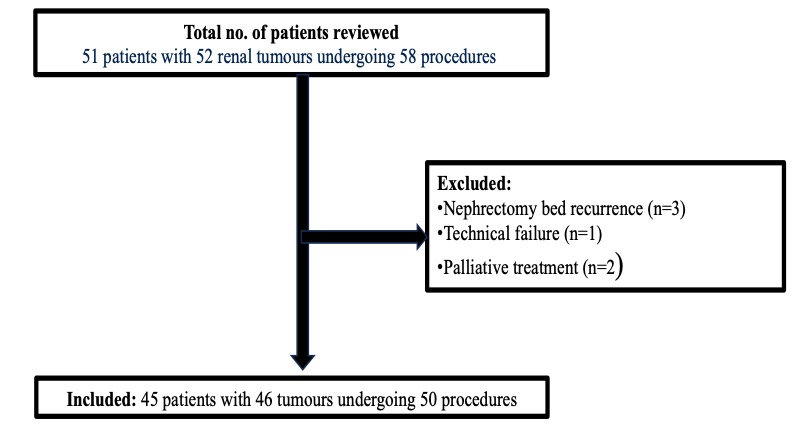
We retrospectively reviewed all patients with biopsy proven RCC who underwent IGTA of a T1 tumour between 1st March 2013 and 1st August 2022. Figure 1. shows the total number of procedures reviewed with the inclusion/exclusion applied. Ablation protocol - RFA was performed with a 2.5cm exposed 17 gauge cluster probe (Medtronic) and 12-minute impedance control ablation program. MWA used a 14 gauge antenna. The type of microwave program used depended on tumour location and size as well as consultant preference and manufacturer guidelines. Cryotherapy used a 14 gauge applicator (Galil) and two freeze thaw cycles with two applicators placed 1 cm apart from each other and 1 cm from the tumour treatment margin. Follow up protocol - Multiphasic renal CT or contrast-enhanced MRI at 3, 6, 9 and 12 months and then annually. This protocol was followed within the confines of the limitation of radiological resources. Data collected included: patient demographics, tumour size and histology, pre and post procedure creatinine, ablation technique, complications, charlston co-morbidity score, length of stay, oncological outcomes, disease free survival and overall survival. Technical success was defined as completion of the treatment protocol. Primary efficacy was defined as the absence of contrast enhancement within the ablated tumour on initial CT or MRI after the first ablative procedure.
Figure 1. Flowchart of patient selection with inclusion criteria applied.
Patient demographics and tumour characteristics are summarized in Table 1. Primary technical success was achieved in 100% of procedures (n=46/46). Primary efficacy was achieved in 94% (43/46 tumours). There was no statistically significant difference in mean pre-procedure creatinine and creatinine one month post-procedure [ 112 mm/l (52-792 mm/l) v 110 mm/l (53-748 mm/l), p = 0.75]. Median length of stay was one day (range 0-13 days). Complications occurred after 8% of ablation procedures (4/50). One patient had an intra-procedure pneumothorax that required a chest drain insertion. The second patient had an intra-procedure haemothorax requiring a chest drain. The third patient developed a perinephric collection at 3 months post ablation that resulted in ipsilateral mild hydronephrosis treated with image-guided drainage and antibiotic treatment as an inpatient on a second unscheduled admission. One patient developed acute urinary retention post procedure. Table 2 compares patient demographics, tumour size and periprocedural outcomes between RFA and MWA. Primary efficacy was greater in the RFA group compared to the MWA group (p=0.02). Larger median RCC diameter was associated with failed primary efficacy in the MWA group (3.8 cm vs 2.4 cm respectively, p= 0.045). Overall survival and local tumour control within 9 years of IGTA are described in Figure 2 and 3, respectively.
Table 1. Patient and tumour characteristics. Note: 1 patient underwent treatment for 2 separate RCC 8 years apart.
Table 2. A comparison of microwave ablation (MWA) and radiofrequency ablation (RFA) group demographics, tumour characteristics and peri-procedural outcomes. Note: 1 patient underwent cryotherapy which is not included in the analysis.
Figure 2. Kaplan Meier graph demonstrating overall survival within 9 years after image guided tumour ablation.
In this study, overall survival at 1, 5 and 9 years was 97.4%, 66.7% and 40% respectively. Local tumour control at 1, 5 and 9 years was 100%, 75% and 50% respectively. In this study, primary efficacy was greater with RFA than MWA. Primary efficacy failure in the MWA group was associated with greater median RCC diameters.
Figure 3. Kaplan Meier graph demonstrating local tumour progression within 9 years after image guided tumour ablation.