MRI appearances of granulomatous prostatitis – our experience of 18 patients and pictorial review
MRI appearances of granulomatous prostatitis – our experience of 18 patients and pictorial review
P Ward, M Sakthithasan, N Raj, S Agrawal, D Paterson, PR Burn
Granulomatous prostatitis (GP) is a rare chronic inflammatory disease of the prostate. Aetiology - idiopathic or due to secondary causes (infection including UTIs and TB), iatrogenic (including TURP), following intra-vesical BCG treatment or associated with systemic granulomatous diseases. Histology - characterized by epitheliod macrophages which may be diffuse (often seen in idiopathic) or clustered (granulomas). Presentation - GP may present with elevated PSA and abnormal DRE and is a great mimic of prostate cancer on MRI.
We reviewed the MRI findings of 18 patients with a histological diagnosis of GP, from a 10-year period, with an incidence of 0.39% (18/4651). Pre-imaging features:- PSA: median 10.3 (range 1.29-28): improved in 75%. PSA density median: 0.15 (range 0.03-0.39) Prior intravesical BCG :27% patients Imaging features:- T2W hypointense: 100% DWI hyperintense (on high b-value): 73% ADC hypointense (<0.1): 87% Moderate/intense enhancement: 95% Collection present: 28% Radiologist’s report considered GP as diagnosis: 17%
Haematoxylin and eosin (a) and triple antibody cocktail (PIN cocktail) staining (b) demonstrating granulomatous prostatitis with an oval granuloma (arrows). The brown staining represents basal cells of an adjacent inflamed duct.
High T2W signal collection: Small high T2W signal collection (red arrow) at prostate apex situated within an adjacent area of low T2W, restricted diffusion and enhancement (orange arrows). Radiologist raised the possibility of granulomatous prostatitis histologically confirmed. Patient presented with abnormal DRE.
Low T2W signal collection: Small collection with low T2W centrally (red arrow), ring enhancing on DCE (also red arrow) situated within a larger surrounding area of low T2W, restricted diffusion and enhancement in the peripheral zone (orange arrows). Histologically confirmed granulomatous prostatitis. Presented with rising PSA, prior BCG therapy. Collections with low T2W signal have been described in caseous necrosis.
High DWI signal collection: Small high DWI signal collection (red arrow) within large multifocal areas of low T2W signal, restricted diffusion and enhancement (orange arrows); granulomatous prostatitis was suggested by the radiologist and confirmed histologically. Presented with recurrent UTIs and positive DRE, PSA 2.
High DWI signal collection:: Small collection (red arrows) with high DWI signal and low-ish ADC in keeping with pus. This is in the peripheral zone with surrounding low T2W signal extending beyond the capsule, mimicking T3a tumour. Granulomatous prostatitis confirmed histologically. Presented with PSA 28, in retention, with firm prostate on DRE.
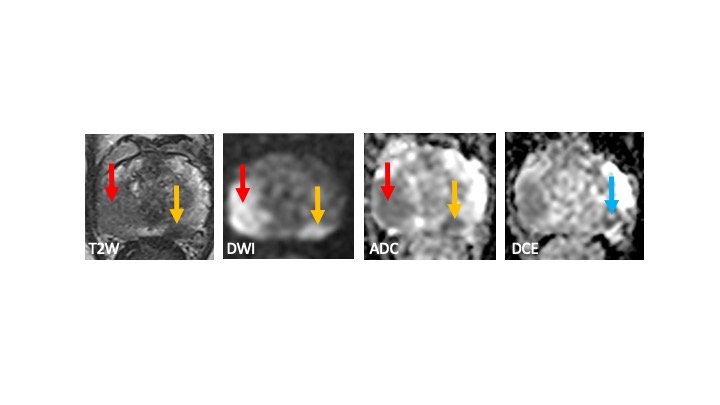
Concurrent tumour and granulomatous prostatitis: Complex case. Large area of abnormal signal right side (red arrows) with low T2W signal and restricted diffusion, histologically confirmed as granulomatous prostatitis. Also, smaller focus of similar signal left peripheral zone (orange arrows), histologically confirmed on targed biopsies as tumour (Gleason 3+4 (10mm 5/6 cores)). In addition, MRI also demonstrated a separate small collection with high ADC (blue arrow). Presented with PSA 10.
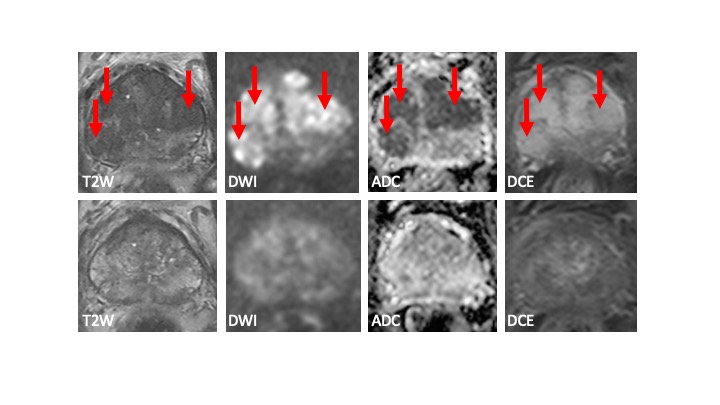
Temporal improvement: Multifocal areas of abnormal signal bilaterally with low T2W signal, marked restricted diffusion and enhancement, mimicking tumour (arrows). Histology demonstrated florid granulomatous prostatitis (same patient as in middle column). Follow-up MRI 6 months later (bottom row) shows marked improvement.
Granulomatous prostatitis mimics prostate cancer on MRI (low T2W, high DWI, low ADC) and biopsy is required for reliable diagnosis. Discriminating features that raise the possibility of granuolomatous prostatitis: Clinical Prior history of intra-vesical BCG, surgical intervention or UTI. Decreased PSA on follow-up. MRI Presence of collections (variously high T2W, low T2W, high DWI). Temporal improvement on follow-up MRI.