MRI Characteristics of Corpus Luteum with Ovarian Oedema: Can both ovaries be affected?
MRI Characteristics of Corpus Luteum with Ovarian Oedema: Can both ovaries be affected?
Kirthi Shamanur, Omar Al Khateeb, Mohan Kumar, Haren E Wijesinghe, Lye Q Hon
Corpus luteum with ovarian oedema (CLOE) is rare and underreported. It usually presents with subacute iliac fossa pain and raised biochemical tumour markers. On imaging, unilateral ovarian enlargement and oedema is present with peripheral follicular displacement and a pseudo-twist of the ovarian vascular pedicle [1]. These features may mimic ovarian torsion or neoplasm. Therefore, it is vital to recognise this rare entity on imaging. In a retrospective study published by Utah University of cases of CLOE (n=243), half of the cohort presented with pelvic pain and 12.9% of findings included enlarged ovaries and displaced follicles, which called for concern for ovarian torsion [2]. Peripheral vascularity of the corpus luteum, evident as enhancement on computerised tomography (CT) or flow signal on Doppler ultrasound (US), is a negative indicator of ovarian torsion [3]. Magnetic resonance imaging (MRI) studies have shown T1-weighted image demonstrating a low intensity lesion and T2-weighted image displaying a heterogeneous high intensity lesion with multiple ovarian follicles located around the periphery of the cortex of the enlarged ovary. This is recognised as a crucial sign of substantial ovarian oedema. A transvaginal ultrasound from the same case also showed several ovarian follicles in the periphery of the ovarian cortex, alongside a solid tumour-like enlarged ovary [6]. The latter can also be evident on MRI findings [4] contributing to the challenges surrounding diagnosis. Furthermore, a case report following 5 patients presenting with ovarian oedema of unknown aetiology showed one cause of ovarian oedema to be hemorrhagic corpus luteum without disrupting blood flow supply [5]. Such features further push diagnosis towards CLOE rather than ovarian torsion. An elevated CA-125 is typically associated with ovarian cancer, however it is also apparent in more common or benign diseases such as uterine fibroids [7], and our case demonstrates CLOE may also be a contributing factor. Explorative laparotomy in a case report, demonstrated a paraovarian cyst and massive ovarian oedema, with no torsion. A partial resection of the ovary was taken and histopathology was normal [6]. However, in a different case, where there was high suspicion of a diagnosis of CLOE, expectant care without surgical intervention was the management of choice, resulting in the progressive resolution of ovarian oedema and the restoration of ovaries to a normal sonographic appearance [5]. Owing to the lack of pathognomonic clinical symptoms, lack of typical hallmarks on imaging and the reliance of final histology, the surgeon's attention has been diverted from performing fertility-sparing surgery on young women.
A 41 year old woman (Gravida 1; Para 1) was referred to Gynaecology with subacute pelvic pain. She suffered from chronic intermenstrual bleeding, dysmenorrhoea and bloating, attributed to multiple uterine fibroids, one of which had been treated surgically (2018). Clinical examination elicited mild left iliac fossa tenderness and routine observations. She underwent an initial urgent MRI, which was reviewed at the gynaecology MDT and a further MRI follow-up 3 months later planned.
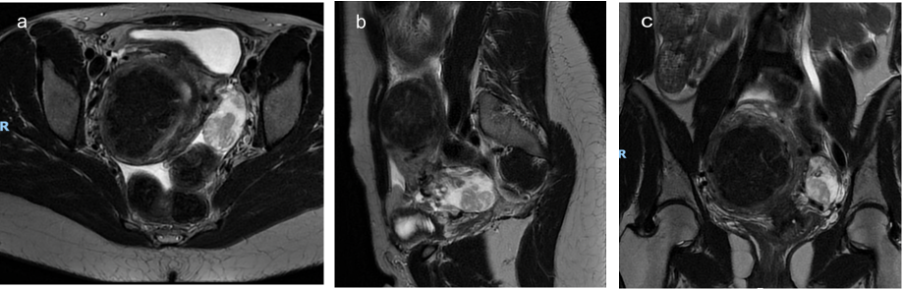
Figure 1: Figure 1a T2 Axial, Figure 1b Sagittal and Figure 1c Coronal High Resolution of initial MRI show diffuse oedema of the left ovarian stroma with heterogeneous soft tissue changes in the inferior aspect.
Figure 2: Figure 2a T1 In-phase, Figure 2b T1 Out-of-phase and Figure 2c T1 Fat Saturation of initial MRI shows heterogeneous T1 isointensity of the left ova ry with no signal loss to suggest intralesional haemorrhage or fat.
Figure 3: Figure 3a B=0, Figure 3b B400, Figure 3c B=800 and Figure 3d ADC Map of initial MRI does not demonstrate diffusion restriction to suggest neoplastic high cellular content.
Blood tests showed a suspicious rise in CA-125 to 111 from 53 (normal range 0 to 35) with remaining normal inflammatory (biochemistry) and germ cell markers, including Alpha Fetoprotein (AFP) and Beta Human Chorionic Gonadotropin (B-HCG). Initial urgent MRI (April 2022) showed a diffusely enlarged left ovary (4.7 x 2.4 cm), with features consistent with peripheral oedema and peripherally displaced ovarian follicles. There was a partial twist to the ovarian vascular pedicle, suggestive of ovarian torsion but no restricted diffusion to indicate malignancy. The right ovary was normal and the uterus was enlarged with the presence of multiple uterine fibroids. There was also a significant volume of free fluid within the pelvis and mild ascites within the upper abdomen. Follow-up MRI (July 2022) showed the left ovary returned to normal MRI characteristics, with an incidental finding of enlarged right ovary (4.9 x 3.2 cm) containing stromal oedema and trace peri-ovarian fluid - similar to the left ovary in the previous study. There were no restricted diffusion or overt sinister features. This time, there was no obvious twist within its vascular pedicle. The uterus remained enlarged with unchanged multiple fibroids. The subsequent MDT outcome was conservative management.
Figure 4: High Resolution Axial T2 follow-up imaging shows normal left ovary with conservative management
Figure 5: Figure 5a and 5b T2 Axial, Figure 5c Coronal and Figure 5d Sagittal High Resolution follow-up MRI show diffuse oedema of the right ovarian stroma with heterogeneous soft tissue changes in the inferior aspect. This was detected incidentally on follow-up of the left ovary
Figure 6: Figure 6a T1 In-phase, Figure 6b T1 Out-phase and Figure 6c T1 Fat Saturation in follow-up MRI shows heterogeneous T1 isointensity of the left ovary with no signal loss to suggest intralesional haemorrhage or fat.
We present for the very first time, to the best of our knowledge, the rapid progression of MRI features of CLOE and interestingly, that it can occur in both ovaries. CA-125 levels were high and both MRIs did not display findings indicative of malignancy. We hypothesise that CLOE may contribute to this raised tumour marker, alongside the pre-existing uterine fibroids. Some features of CLOE are apparent on ultrasound, however given the pre-operative role of MRI and the high margin of error concerning the diagnosis, we opted for an MRI. The key difference between both MRI findings was the twist within the vascular pedicle on the first MRI, which created suspicion towards ovarian torsion. Within 3 months, there was no obvious twist and the enlarged oedematous left ovary on the initial MRI had completely resolved, with the findings having shifted to the right ovary. Diagnosis of CLOE is evidently challenging. Therefore, through this case report, we aim to further contribute to the limited understanding and research of this benign ovarian pathology, to aid in achieving a clearer diagnosis via MRI, therefore preventing unnecessary invasive procedures. References: 1. Chang HC, Bhatt S, Dogra VS. Pearls and pitfalls in diagnosis of ovarian torsion. RadioGraphics. 2008;28(5):1355-1368. doi:10.1148/rg.285075130 2. Rogers D, Al-Dulaimi R, Rezvani M, Shaaban A. Corpus luteum with ovarian stromal edema is associated with pelvic pain and confusion for ovarian torsion. Abdom Radiol (NY). 2019;44(2):697-704. doi:10.1007/s00261-018-1781-z 3. Rogers D, Al-Dulaimi R, Rezvani M, Kennedy A, Shaaban A. Peripheral hypervascularity of the corpus luteum with ovarian edema (CLOE) may decrease false positive diagnoses of ovarian torsion. Abdom Radiol (NY). 2019;44(9):3158-3165. doi:10.1007/s00261-019-02091-3 4. Tamai K, Koyama T, Saga T, et al. MR features of physiologic and benign conditions of the ovary. Eur Radiol. 2006;16(12):2700-2711. doi:10.1007/s00330-006-0302-6 5. Beyth Y, Klein Z, Tepper R, Weinstein S, Aviram R. Hemorrhagic corpus luteum is associated with ovarian edema. J Pediatr Adolesc Gynecol. 2006;19(5):325-327. doi:10.1016/j.jpag.2006.06.002 6. Bischof P, Galfetti MA, Seydoux J, von Hospenthal JU, Campana A. Peripheral CA 125 levels in patients with uterine fibroids. Human Reproduction. 1992Jan;7(1):35–8. 7. Umesaki N et al. Sonographic charac-teristics of massive ovarian edema. Ultrasound in obstetrics & gyneco-logy, 2000, 16(5):479–81.
Figure 7: Figure 6a B=0, Figure 6b B400, Figure 6c B=800 and Figure 6d ADC Map in follow-up MRI does not demonstrate diffusion restriction to suggest neoplastic high cellular content.